EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 1642
HTML: 249
PDF: 737
|
Introduction: Colonoscopy is a useful tool in modern medicine and is increasingly employed for both diagnostic and treatment purposes. However, bowel preparations can cause electrolyte imbalance, with the risk apparently related to the type of bowel cleansing solution used, the age of the patient and their comorbidities. Symptomatic hyponatremia, especially coma, is a rare complication of oral bowel preparation for colonoscopy and is thought to result from excessive antidiuretic hormone secretion.
Case description: The authors report the case of a 48-year-old man who developed symptomatic hyponatremia (coma) after bowel preparation with sodium picosulfate/magnesium oxide/citric acid prior to a colonoscopy. The patient was admitted to an intensive care unit where other causes of coma were excluded. The symptoms of hyponatremia rapidly resolved after sodium level correction with intravenous administration of hypertonic saline.
Discussion: Hyponatremic coma is an uncommon but serious complication of colonoscopy bowel preparation. Patients at risk (>65 years old, chronic kidney disease, heart failure, history of electrolyte problems, or taking thiazide diuretics, angiotensin-converting-enzyme inhibitors or antidepressants) should be closely monitored during bowel cleansing and macrogol-based solutions should preferably be used.

|
Views: 1250
HTML: 98
PDF: 408
|
We describe the case of an 84-year-old woman who presented with right lower chest pain, anaemia and newly deranged liver function which was followed by massive upper gastrointestinal (GI) bleeding with no source of bleeding found on upper GI endoscopy. CT angiography of the GI tract confirmed rupture of a pseudoaneurysm of the right hepatic artery (RHA) that was treated successfully with trans-arterial embolization of the RHA.

|
Views: 1020
HTML: 288
PDF: 447
|
A 73-year-old woman with a diagnosis of vulvar carcinoma submitted to curative surgery 5 years previously, presented to the emergency department with prostration and vulvar haemorrhage. Although the gynaecological examination was unremarkable, she had a mass in the left chest wall and hypercalcemia. A CT scan of the thorax revealed a voluminous left hemithorax mass invading the mediastinum, lung, pleura and chest wall. Ultrasound-guided biopsy of the mass showed infiltration by a well-differentiated keratinizing squamous cell carcinoma (SCC). This case report describes an extremely rare metastatic pattern in vulvar SCC concomitant with paraneoplastic hypercalcemia.
|
Views: 927
HTML: 157
PDF: 438
|
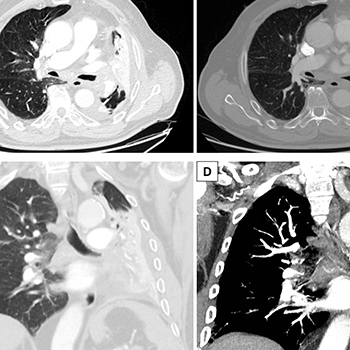
Pancreatic pseudocysts are a frequent complication of chronic pancreatitis. Nonetheless, they seldom extend beyond the peripancreatic region. However, migration towards the mediastinum may cause heterogeneous and non-specific symptoms, such as dysphagia, chest pain and dyspnoea, which depend on the localization and extension of the cysts. We present the case of a patient with chronic pancreatitis who was admitted to our ward for low-grade fever and mild dyspnoea and who rapidly developed bilateral laterocervical swelling associated with acute dyspnoea and trismus. A total body CT scan showed multiple abdominal pancreatic pseudocysts, one of which had migrated to the mediastinum and towards the retropharyngeal space. Clinicians should always consider the possibility of extra-pancreatic pseudocysts in patients with known pancreatitis so that uncommon clinical presentations with a potentially fatal outcome will be recognized.
|
Views: 923
HTML: 116
PDF: 494
|
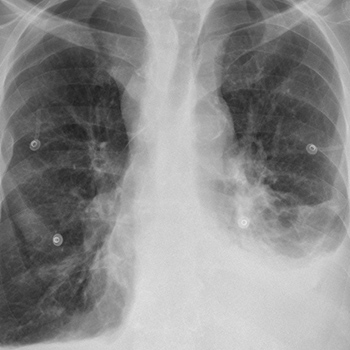
Non-Hodgkin lymphomas are rare causes of primary lung neoplasms and most are B-cell in origin. Anaplastic large cell lymphoma is an exceedingly rare type of primary pulmonary lymphoma, with an aggressive clinical course.
We present the case of an 85-year old male patient who attended our Emergency Department complaining of respiratory and constitutional symptoms, and who was found to have a bronchial mass causing subtotal atelectasis of the left lung. Histological examination showed an anaplastic large cell lymphoma and further investigation revealed that it was limited to the lung. To our knowledge, very few similar cases have been reported in the literature.

|
Views: 1387
HTML: 413
PDF: 639
|
Bullous pemphigoid is a chronic autoimmune blistering disease. Recently, several reports suggested dipeptidyl peptidase 4 (DPP-4) inhibitors, also known as gliptins, were a potential cause of drug-induced bullous pemphigoid but not of both bullous pemphigoid and alopecia areata together. Here we describe the case of a 68-year-old man with type 2 diabetes mellitus who developed new onset diffuse alopecia on the scalp with diffuse tense bullae over his body a few months after linagliptin was introduced for better control of his diabetes.
DPP-4 inhibitors are not known to increase the risk of alopecia. To the best of our knowledge, this is the first report of linagliptin-associated alopecia areata and bullous pemphigoid, which may help demonstrate if there are any links between DPP-4 inhibitors and alopecia.
|
Views: 1394
HTML: 133
PDF: 559
|
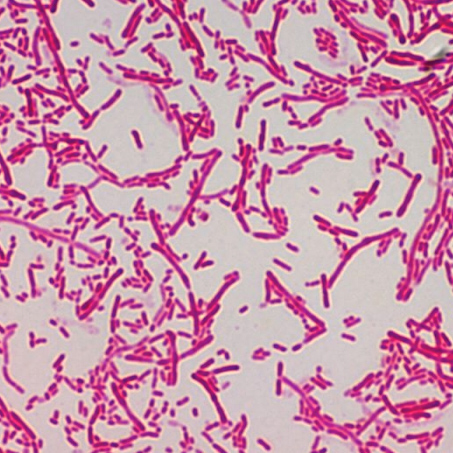
We present the case of a 75-year-old woman admitted to hospital because of an infected pressure ulcer. Cultures revealed that the responsible bacterium was Sphingobacterium multivorum, which was successfully eradicated with ciprofloxacin. Over the last few years, there have been reports of new cases of infection caused by bacteria previously not thought to be harmful to humans, like S. multivorum. Previous cases were reported mostly in immunosuppressed patients and the present report is, to our knowledge, the first describing a pressure ulcer infected by this bacterium.

|
Views: 1180
HTML: 153
PDF: 589
|
AA amyloidosis is a rare complication of chronic inflammatory disorders and has been associated with rheumatoid arthritis and ankylosing spondylitis.
We present a case of AA amyloidosis secondary to Sjogren’s syndrome (SS). A 79-year-old woman presented with rapidly progressive renal failure and complaints of asthenia, anorexia and generalized oedema. She had severe renal failure (creatinine 6.0 mg/dl), with microscopic haematuria, nephrotic proteinuria and low serum albumin levels, and an increased erythrocyte sedimentation rate. Serum protein electrophoresis revealed a peak in the gamma globulin zone. The patient was started on haemodialysis and corticosteroids. Clinical results showed the patient met the diagnostic criteria for primary SS, and neoplastic haematological disease was excluded. Renal biopsy revealed a diagnosis of AA amyloidosis.
Renal AA amyloidosis is a rare condition in patients with primary SS. However, in patients with proteinuria and/or renal failure, it should be included in the differential diagnosis and a renal biopsy should be performed.

|
Views: 4191
HTML: 50574
PDF: 782
|
Achenbach’s syndrome, also known as paroxysmal finger haematoma, is a rare condition that results in spontaneous bruising and pain in one or more fingers. Despite its benign and self-limiting course, the remarkable clinical presentation can suggest serious vascular and haematological disease leading to unnecessary referrals and invasive investigations. The authors present the case of a 60-year-old woman with an acute painful and bruised finger. All other physical findings and investigations were normal, except for autoimmune thyroiditis. Based on the clinical presentation and course, the diagnosis of Achenbach’s syndrome was made and the symptoms resolved without treatment.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

