EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 2261
HTML: 224
PDF: 352
Copyright Form: 0
Disclosure form: 0
Figure 1: 0
|
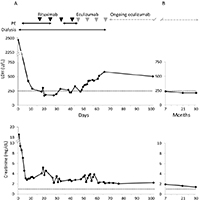
Objectives: To describe the diagnosis and treatment of a severely ill patient presenting with thrombotic microangiopathy (TMA) of unknown cause.
Case presentation: An adult female presented to intensive care with abdominal pain and haemorrhagic shock, requiring reanimation.
Results: Features of TMA were present, but initial plasma exchange was ineffective. Treatment with the anti-C5 antibody, eculizumab, improved laboratory parameters and organ function, albeit slowly. Eculizumab remains effective and well tolerated after 30 months of treatment.
Conclusion: This case demonstrates the complexities and importance of early identification of atypical haemolytic uraemic syndrome in patients presenting with TMA.

|
Views: 895
HTML: 1084
PDF: 471
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
Disclosure form and copyright authorisation form: 0
|
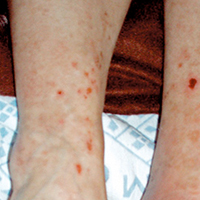
Objectives: We report an atypical presentation of eosinophilic fasciitis and provide a concise overview of the literature.
Materials and Methods: Clinical and laboratory findings in a patient presenting with fever and skin induration were recorded. A deep muscle biopsy was performed in order to confirm the diagnosis.
Results: A spontaneous favourable clinical and radiological evolution was observed.
Conclusion: The diagnosis of eosinophilic fasciitis is challenging due to the lack of pathognomonic signs and symptoms. As spontaneous resolution has been described, watchful waiting is defendable depending on the clinical presentation. Although magnetic resonance imaging (MRI) can be useful in establishing the diagnosis, a deep muscle biopsy remains the gold standard diagnostic tool.
|
Views: 1363
HTML: 246
PDF: 446
Author Information Page: 0
Copyright Transfer and Conflict of Interests: 0
|
A case of non-fatal drowning with a successful outcome despite a submersion time of 25 min is described. Our case report emphasizes the role of accidental hypothermia in the survival of drowning victims with hypoxic brain injury, and supports the use of therapeutic hypothermia in the resuscitation of these patients.
|
Views: 770
HTML: 233
PDF: 365
|
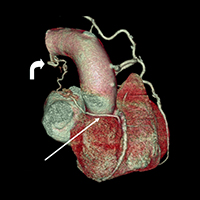
Coronary artery fistulae (CAF) are a rare entity describing abnormal communication between a coronary artery and cardiac chamber or a large intrathoracic vessel and are seldom described in the literature[1]. These fistulae can be either congenital or acquired. Often incidental in finding, CAFs can have serious clinical sequelae, and should be duly reported and discussed with the cardiac team. More than 50% of patients with CAFs may be asymptomatic; 34% may report chest pain; 13% may have symptoms of heart failure, and a minority of 2% may suffer from endocarditis and arrhythmias[2]. The largest series to our knowledge was reported by the Cleveland Clinic, which found 225 patients with incidental CAF out of 126,595 coronary catheterizations (incidence of 0.18%), performed during a span of 28 years [3].
Multiple CAFs are an even rarer entity and only a handful of cases have been reported in the literature to date. Few cases of double CAFs have been reported that describe two different feeder coronary arteries giving rise to separate drainage sites[3]. In our report, however, we describe a new entity: a single-feeder coronary vessel communicated with two drainage sites. Our case is curiously unique, in which we report a single artery, originating from the right coronary artery (RCA) with double drainage sites – one to the left pulmonary artery and the second to the left bronchial artery.

|
Views: 1161
HTML: 1258
PDF: 461
cover letter: 0
figure 1: 0
figure 2: 0
title page: 0
|
Acupuncture has been used therapeutically for thousands of years and is considered a relatively safe procedure. Sternoclavicular joint (SCJ) arthritis is a rare joint infection and has never been reported as an adverse event of acupuncture. We report the case of a 50-year-old woman who presented with progressive left neck, shoulder and upper chest pain after acupuncture. A computerized tomography (CT) scan revealed septic arthritis over the left sternoclavicular joint (SCJ) and methicillin-sensitive Staphylococcus aureus bacteraemia was noted. The patient was discharged uneventfully after intravenous antibiotic treatment. SCJ septic arthritis should be considered if unilateral neck and upper chest pain occurs after acupuncture.

|
Views: 807
HTML: 852
PDF: 346
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
Untitled: 0
|
Objectives: Extensive calcinosis in a patient with dermatomyositis is a rare clinical presentation in adults. The aim of this report is to present the clinical and radiographic features of a 25-year-old woman with dermatomyositis and extensive calcinosis.
Case Presentation: A 25-year-old woman with extensive calcinosis on background dermatomyositis is described.
Results: The clinical and radiographic features of the patient were consistent with dermatomyositis complicated by extensive calcinosis in an adult.
Conclusion: Dermatomyositis with extensive calcinosis is a rare clinical presentation in adults.
|
Views: 727
HTML: 1730
PDF: 364
Figure 1: 0
Figure 2: 0
Figure 3: 0
Figure 4: 0
Figure 5: 0
Table 1: 0
Author information page: 0
|
Objectives: To highlight systemic involvement features in Sjögren Syndrome (SS).
Materials and methods: A case of a 32-year-old woman presenting with flaccid tetraparesis, in the setting of severe hypokalaemia, is described.
Results: Additional evaluation confirmed primary SS with type 1 renal tubular acidosis (RTA1) and gammaglobulin-mediated vasculitis. A significant clinical improvement was achieved following adequate treatment.
Conclusion: Extra-glandular involvement in SS is usually due to autoimmune lymphocytic infiltration and severe complications can be avoided if there is a prompt diagnosis.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

