EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 227
HTML: 19
PDF: 126
|
Inappropriate therapy is a frequent adverse consequence of implantable cardioverter-defibrillator. Inappropriate therapy often occurs due to the misinterpretation of sinus tachycardia or atrial fibrillation/flutter with rapid atrioventricular conduction by the device. Current implantable cardioverter-defibrillator (ICD) mechanisms integrate various discriminators into algorithms to differentiate supraventricular tachycardia (SVT) from ventricular tachycardia (VT), to prevent such occurrences. A 40-year-old man suffered seizures and cardiac arrest abruptly, without prior complaints of chest pain. Without delay, he initiated cardiopulmonary resuscitation (CPR), resulting in the regaining of spontaneous circulation. The patient had previously received a single-chamber ICD due to recurring VT and a prior episode of cardiac arrest. The patient had a medical background of coronary artery disease with complete revascularisation and no previous occurrence of SVT. Interrogating the ICD revealed captured non-sustained ventricular tachycardia (NSVT) and SVT events but no VT episode or shock therapy. During the specified time period, the patient underwent an electrophysiological study, and no SVT was induced with the normal function of the atrioventricular and sinoatrial nodes. Various causes can lead to errors in morphology discrimination criteria in single-chamber ICDs. Extending the detection interval is highly recommended to avoid misclassification of ICDs.

|
Views: 240
HTML: 28
PDF: 135
|
Addison’s disease is a rare, autoimmune condition leading to the destruction of the adrenal gland. Autoimmune conditions are known to commonly co-occur. When Addison’s disease presents in the setting of autoimmune thyroid disease and/or type 1 diabetes, this condition is termed autoimmune polyendocrine syndrome type II, a rare endocrinopathy found in roughly 1.4-4.5 per 100,000 individuals. Here, we describe a clinical case presenting with hypotension refractory to fluid resuscitation and electrolyte derangements later diagnosed as autoimmune polyendocrine syndrome type II.

|
Views: 265
PDF: 165
HTML: 12
|
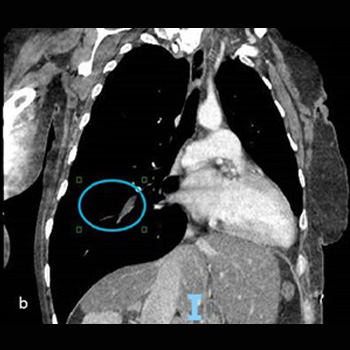
Anomalous bronchial artery origins may have clinical implications beyond their anatomical curiosity. In this case, the identification of such an anomaly led to the diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH).
A 49-year-old male with a history of recurrent deep vein thrombosis (DVT) and pulmonary embolism (PE) on anticoagulation presented with chest pain and shortness of breath. Laboratory analysis was remarkable for a troponin peak of 14.74 ng/ml, a brain natriuretic peptide level of 602 pg/ml and a D-dimer level of 0.62 µg/ml. Electrocardiogram showed non-specific ST elevation in the anterolateral and inferior leads. Computed tomography angiography (CTA) of the chest was positive for PE involving the right lower lobe pulmonary arterial tree. Echocardiogram showed reduced left ventricular function (ejection fraction 38%) and akinesis of the antero-apical and infero-apical segments. Cardiac catheterization revealed non-obstructive coronary arteries, and an anomalous origin of a right bronchial artery from the right coronary artery. The right bronchial hypertrophied as it supplied collateral flow to the occluded right pulmonary artery. This anomaly and the patient’s history of multiple DVT/PEs while on therapeutic levels of warfarin with near normal D-dimer levels raised suspicion for a false positive PE. Pulmonary angiogram revealed chronic occlusion in branches of the right pulmonary artery, mean pulmonary artery pressure of 36 mmHg and no acute thrombus. Ventilation-perfusion scan confirmed the diagnosis of CTEPH. The patient underwent successful pulmonary thromboendarterectomy and subsequently had normalization of mean pulmonary artery pressure.
This case underscores the importance of a comprehensive diagnostic approach, and consideration of alternative explanations for imaging findings, that unveiled the diagnosis of a complex and life-threatening condition such as CTEPH.

|
Views: 234
HTML: 10
PDF: 93
|
Hepatitis A is a mild self-limiting infection of the liver with spontaneous resolution of symptoms in most cases. However, clinicians should be aware of some commonly encountered complications and extrahepatic manifestations associated with hepatitis A for timely diagnosis and treatment. Rhabdomyolysis, an exceedingly rare complication of hepatitis A, is scarcely documented. We present a case of a 64-year-old man with symptoms consistent with rhabdomyolysis and an evanescent rash secondary to acute hepatitis A. He eventually recovered with conservative management. This case emphasizes the importance of recognizing and treating atypical presentations of acute hepatitis A infection.

|
Views: 214
HTML: 11
PDF: 110
|
Bronchial artery embolization (BAE) is a procedure that aims to control bleeding from bronchial arteries in massive and chronic haemoptysis. It is considered to be a life-saving measure in severe life-threating haemoptysis. Although it is minimally invasive and has a high success rate, it still carries a list of complications. These include post-embolisation syndrome, chest pain, back pain, dysphagia, vascular injury at the site of the embolisation leading to dissection, perforation, pseudoaneurysm and, very rarely, embolic infarction to non-target vessels.
Stroke is one of the rare complications post BAE, and it can be severe and fatal. Few cases of stroke post BAE have been reported in the literature, and they were mainly due to posterior cerebral circulation infarction. Here, we report a case of a stroke post BAE due to massive middle cerebral artery (MCA) infarction and to our knowledge it seems to be the first reported case of MCA infarction post BAE.
The discussion will cover the possible mechanisms of embolic passage, the outcome of the case including rehabilitation perspectives and the learning points. These will also highlight the importance of early recognition, which can save patients from a disabling stroke in the future.

|
Views: 154
HTML: 21
PDF: 81
|
Khat is a plant that is commonly used for its stimulating effects and is chewed for its psychoactive properties. It creates feelings of euphoria that are similar to when taking amphetamines. There is an association between khat and liver injury, but the mechanism is not well known. We present three cases of khat-induced liver injury. All cases have elevated IgG and either positive antinuclear antibodies (ANA) or anti-smooth muscle antibody (ASMA); each case has a different course and requires different management. One case improved only by stopping khat, one required a short course of steroids and the last case required treatment such as that for autoimmune hepatitis (AIH).

|
Views: 421
HTML: 24
PDF: 252
|
Euglycemic diabetic ketoacidosis (euDKA) is a rare but severe metabolic complication of diabetes mellitus characterised by elevated anion gap metabolic acidosis despite normal or mildly elevated blood glucose levels. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have emerged as effective antidiabetic medications, yet their use is associated with an increased risk of euDKA, especially when coupled with insulin dose reduction.
We present the case of a 50-year-old male with a 20-year history of diabetes mellitus, initially managed with insulin and metformin, who developed euDKA following the introduction of empagliflozin and sitagliptin alongside a reduction in insulin therapy. Despite normoglycaemia the patient exhibited symptoms of ketoacidosis, including chronic fatigue, polydipsia, and polyuria.
Diagnostic workup revealed metabolic acidosis, elevated inflammatory markers, acute kidney injury and ketonuria. Subsequent specialised laboratory tests confirmed type 1 diabetes mellitus (T1DM) with the presence of anti-glutamic acid decarboxylase (anti-GAD) antibodies and the absence of C-peptide secretion. Management involved fluid therapy, intravenous insulin and glucose administration.
This case underscores the diagnostic challenges of euDKA and emphasises the importance of differentiating between T1DM and T2DM, as management strategies vary significantly. Patient education on insulin therapy and injection techniques is crucial to prevent complications such as improper insulin delivery and dose reduction, which can precipitate euDKA.
In conclusion, clinicians should be vigilant for euDKA in patients on SGLT2 inhibitors, particularly when insulin dose reduction is involved. Comprehensive patient education and accurate differentiation between diabetes types are essential for timely diagnosis and optimal management, thereby reducing the risk of severe complications.

|
Views: 313
HTML: 14
PDF: 171
|
Background: A case of bilateral multifocal serous retinal detachments and dry eye complicated with unilateral peripheral ulcerative keratitis (PUK) during erdafitinib therapy is described.
Case description: A 76-year-old male underwent a baseline examination two months after initiating 8 mg erdafitinib therapy (April 2023) due to metastatic urothelial carcinoma. Left subfoveal serous retinal detachment was observed initially but the treatment was resumed as he was asymptomatic. In May 2023, bilateral multifocal subretinal fluid pockets were identified, and the patient was still asymptomatic. However, in June 2023 he complained of bilateral redness and a stinging sensation in his right eye. Bilateral severe dry eye and right PUK were diagnosed. He was prescribed dexamethasone eye drops and sodium hyaluronate artificial tears for both eyes. One week later corneal staining decreased, and progression of PUK ceased. Erdafitinib therapy was discontinued in June 2023 due to the planned transurethral prostatectomy. By July 2023, after discontinuation of the drug and administration of the topical treatment, the dry eye improved and the PUK became inactive. There was also resolution of subretinal fluid pockets in the right eye and a reduction of subretinal fluid pockets in the left eye. After the reinitiation of erdafitinib therapy, serous retinal detachments recurred in both eyes in September 2023, but both corneas remained stable with topical low-dose dexamethasone, cyclosporine-A and artificial tear usage.
Conclusion: Erdafitinib therapy may lead to concurrent anterior and posterior segment complications. Multidisciplinary monitoring is crucial for patients undergoing erdafitinib therapy to prevent possible visual disturbances.

|
Views: 209
HTML: 20
PDF: 166
|
Introduction: Ventricular septal defect (VSD) is a severe complication following acute myocardial infarction (MI) resulting from mechanical disruption of the interventricular septum due to extensive myocardial necrosis. Despite advances in management, the mortality rate approaches 50%. We report a case of a 58-year-old male with VSD following MI who was successfully treated with a delayed surgical approach after haemodynamic support using Impella.
Case description: A 58-year-old man with type 2 diabetes mellitus and hypertension presented with three days of chest pain. Testing revealed late presenting acute anterior ischaemic infarction and left-to-right shunt in the apical ventricular septum. Urgent cardiac catheterisation showed near-total occlusion of the left anterior descending artery. An Impella CP® was placed before angioplasty with a drug-eluting stent to optimise haemodynamics. After a multidisciplinary discussion, the Impella CP® was upgraded to Impella 5.5®, and surgery was delayed allowing for scar formation. The patient remained in the intensive care unit, where he underwent physical therapy, showing improvements in exercise tolerance by the time of surgery. He underwent a left ventriculotomy with a successful repair via an endocardial patch 28 days after initial presentation. Post-operative recovery was uneventful, with the patient discharged five days later, reporting no physical limitations one month post-discharge.
Conclusion: The successful management of VSD post-MI relies on interdisciplinary collaboration, careful timing of surgical intervention and the strategic use of mechanical support devices such as the Impella. This case highlights the potential for favourable outcomes when tailored treatment approaches are employed.

|
Views: 358
HTML: 21
PDF: 162
|
Background: Vaccine-induced immune thrombotic thrombocytopenia (VITT) is a rare life-threatening thrombotic reaction to COVID-19 vaccines.
Case description: Two young male first cousins, with a family history of idiopathic thrombocytopenic purpura, developed VITT after the Ad26.COV2.S vaccine. Both had a favourable clinical and analytical outcome. We investigated the genetic factors that could be associated with a genetic predisposition to VITT.
Conclusions: There are no published cases where the VITT patients were relatives. The genetic study did not reveal any likely pathogenic variants, although the prevalent polymorphism c.497A>G (p.(His166Arg)) in the FCGR2A gene was found in a homozygous state. More studies are required to better understand VITT’s pathophysiology and any underlying genetic predispositions.

|
Views: 235
HTML: 10
PDF: 126
|
Background: Alagille syndrome (ALGS) is a multisystem disorder involving at least three systems among the liver, heart, skeleton, face, and eyes. Common cardiac associations include pulmonary artery stenosis/atresia, atrial septal defect (ASD), ventricular septal defect (VSD) and tetralogy of fallot (ToF). Coarctation of aorta (CoA), renal and intracranial arteries are commonly involved vessels in Alagille syndrome. We present two cases with rare cardiovascular manifestations of Alagille syndrome.
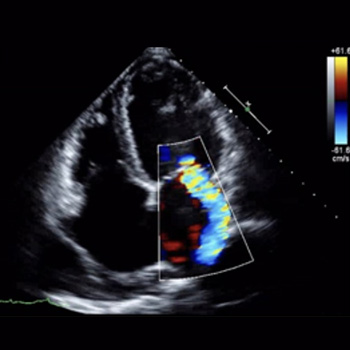
Case description: Case 1: A 25-year-old female with a history of Alagille syndrome presented to the cardiologist office for progressive exertional dyspnoea, orthopnoea, and palpitations. She was tachycardiac on examination and had an apical diastolic rumble. A transthoracic echocardiogram (TTE) showed a left ventricular ejection fraction (LVEF) of 60% and parachute mitral valve (PMV) with severe mitral stenosis. A transoesophageal echocardiogram (TOE) showed insertion of chordae into the anterolateral papillary muscle, severe mitral stenosis with a valve area of 0.7 cm. She was referred to a congenital heart disease specialist and underwent robotic mitral valve replacement with improvement in her symptoms.
Case 2: A 27-year-old female with known Alagille syndrome and resistant hypertension presented to the cardiologist office due to progressive exertional dyspnoea for a year. She was hypertensive and had a new 2/6 systolic ejection murmur along the left upper sternal border. TTE revealed an LVEF of 60% and pulmonary artery pressure of 19 mmHg. A CoA was suspected distal to the left subclavian artery due to a peak gradient of 38 mmHg. Cardiac magnetic resonance (CMR) imaging ruled out CoA, and diffuse narrowing of the descending thoracic aorta measuring 13–14 mm in diameter was noted. The patient was referred to a congenital heart disease specialist for further management.
Conclusion: PMV presenting as mitral stenosis and mid-aortic syndrome are not commonly described anomalies in association with Alagille syndrome. TTE, TOE and CMR played a key role in diagnosis and management of these patients.

|
Views: 312
HTML: 64
PDF: 167
|
The incidence of post-infectious autoimmune diseases has been on the rise following the COVID-19 pandemic. Recently, an autistic patient was admitted to the hospital presenting with a mild upper respiratory system COVID-19 infection. Months after recovery and polymerase chain reaction negativity, the patient developed HEp-2 cell positivity and presented with relapsing polychondritis (RP), a rare autoimmune disease. The mechanism of this autoimmune invasion is ultimately caused by activating a myriad of immune reactions. Lymphocytopenia almost always accompanies various clinical forms of COVID-19; however, it may drive the lymphocytopenia-induced proliferation of autoreactive T cells via the activation of interleukin-6 (IL-6). Moreover, high levels of neutrophils during infection promote autoimmune disease by releasing cytokine and chemokine cascades that accompany inflammation, and neutrophil extracellular traps regulating immune responses through cell–cell interactions. Furthermore, autism spectrum disorder patients display an altered immune system that includes an augmented inflammatory cytokine milieu leading to an increased pro-inflammatory Th1/Th2 ratio. In addition, the pathophysiology of RP is majorly associated with a cell-mediated immune reaction; thus, the predisposing exaggerated immune system of such patients must also be considered as a predisposing factor to the development of post-infectious autoimmune diseases.

|
Views: 261
HTML: 14
PDF: 167
|
Introduction: Blue rubber bleb nevus syndrome is a rare disorder of venous malformations, with around 200 cases reported. We present a case of Mycobacterium xenopi infection in a patient with blue rubber bleb nevus syndrome.
Case Description: A 40-year-old female with blue rubber bleb nevus syndrome, asthma, and bronchiectasis came to the pulmonology clinic with shortness of breath and a cough. She was recently admitted for a bronchiectasis exacerbation but continued to have a worsening productive cough and fevers. The most recent CT scan of the chest showed interval stable right upper lobe fibrocavitary disease, demonstrating gradual progression over two years. She had occasional positive cultures for Mycobacterium Avium Complex and M. xenopi one year previously, assumed to be a colonizer and not treated. Most recent hospital cultures were negative for bacteria and an acid-fast bacilli smear. She was sent to the emergency department for bronchiectasis exacerbation and returned to the clinic six weeks later with two sputum cultures growing M. xenopi. It was decided to treat M. xenopi as this was likely the cause of her cavitary lung lesion and frequent infections. Azithromycin, rifampin, and sulfamethoxazole/trimethoprim were initiated. Intravenous amikacin was added later on. She finally had a right partial lung resection done after one year at an outside hospital. She was on and off antibiotics for M. xenopi for approximately three years with negative repeat cultures for non-tuberculous mycobacteria.
Conclusion: Due to the high mortality of M. xenopi infections (which can be as high as 69%), treatment of at least twelve months is recommended. To our knowledge, this is the first reported case of M. xenopi in a patient with blue rubber bleb nevus syndrome.
|
Views: 222
HTML: 12
PDF: 136
|
Introduction: Orthotopic heart transplantation is the gold standard for the treatment of advanced heart failure in the absence of contraindications. Infective endocarditis is a rare complication in patients after heart transplantation. The treatment of endocarditis after heart transplantation is challenging since there is a need for ongoing immunosuppression.
Case description: We present the case of a 51-year-old orthotopic heart transplant recipient enrolled in a chronic dialysis program, in whom we diagnosed and successfully treated recurrent infective endocarditis of the mitral valve caused by Enterococcus and Enterobacter species. Despite the complicated course of the disease, the treatment was successful.
Conclusions: Recurrent infective endocarditis after heart transplantation can be treated successfully with a multidisciplinary approach and robust antimicrobial therapy.

|
Views: 213
HTML: 12
PDF: 160
|
Introduction: EML4-ALK is an oncogenic driver, seen in around five per cent of advanced non-small-cell lung cancer (NSCLC) patients, which can be targeted with anaplastic lymphoma kinase tyrosine kinase inhibitors with great response rates. Disease flare refers to sudden rapid disease worsening on tyrosine kinase inhibitors (TKI) discontinuation, which is associated with shorter survival and worse outcomes. Here, we review cases previously published in the literature where patients developed disease flares, and contrast this with our patients who had prolonged survival despite TKI discontinuation.
Case description: We report three different patients with advanced ALK-positive NSCLC seen at our institute, who had EML4-ALK translocation variant 1 oncogenic driver on next-generation sequencing. They received treatment with several different ALK inhibitors before opting to discontinue TKI. They were able to come off TKI safely without developing disease flare and had prolonged survival.
Discussion: Shorter time to progression on TKI, presence of symptoms with disease progression or central nervous system/pleural metastasis have been previously linked with development of flare, although this was not seen in our case series. Tumour response at the time of treatment discontinuation, line of therapy, overall disease burden, fusion variant and co-alteration status can affect the prognosis of these patients after ALK TKI cessation. In particular, variant 1 and wild-type TP53 status may be a suitable patient population for dose optimisation strategies. Intermittent TKI dosing strategies may help to avoid acquiring resistance mutations and prevent long-term treatment toxicities.
Conclusion: It is important for clinicians to identify patients at risk for developing disease flare on TKI discontinuation to improve outcomes. Intermittent TKI dosing strategies require further investigation.

|
Views: 173
HTML: 12
PDF: 146
|
Late onset combined immunodeficiency (LOCID) is a rare variant of common variable immunodeficiency (CVID), typically affecting adult patients who present with opportunistic infections (OI) and/or low CD4+ T lymphocytes. Diagnostic delay is common due to the rareness of this entity, increasing morbidity and mortality. We report on a 66-year-old male who developed a severe gastrointestinal cytomegalovirus (CMV) infection, refractory to antiviral treatment and anti-cytomegalovirus specific human immunoglobulin administration, with a fatal outcome due to an undiagnosed LOCID.

|
Views: 219
HTML: 12
PDF: 151
|
Background: Wellens’ syndrome is characterised by a history of chest pain with an abnormal electrocardiogram (EKG), demonstrating biphasic or deeply inverted T waves in leads V2–3 (may extend to involve all precordial and lateral limb leads – the type B Wellens’ pattern). A Wellens’ EKG pattern is considered highly specific for critical stenosis involving the ostial/proximal left anterior descending artery (LAD). However, there are no reported cases of an association of a Wellens’ EKG pattern with myopericarditis. Here, we present such a rare case.
Case description: A thirty-one-year-old female with known essential hypertension and psoriatic arthritis presented with a constant, central chest pain radiating to the shoulders and back. The patient’s physical examination was unremarkable at presentation other than elevated blood pressure at 170/68 mmHg. An EKG at presentation demonstrated deep symmetric T-wave inversions in anterolateral leads with elevated high-sensitivity troponin, and an elevated erythrocyte sedimentation rate. The patient was referred to the cardiac catheterisation laboratory for concerns of a Wellens’ EKG pattern; however, invasive angiography demonstrated only obtuse marginal branch disease – no LAD disease was noted. Cardiac magnetic resonance (CMR) imaging confirmed the diagnosis of myopericarditis and absence of myocardial infarction. The patient was medically managed and discharged home in a stable condition.
Conclusion: In literature and established clinical practice, the Wellens’ EKG pattern is considered highly concerning for critical ostial/proximal LAD stenosis. However, we now propose that myopericarditis may be considered in a differential diagnosis for this EKG pattern.

|
Views: 186
HTML: 14
PDF: 125
|
Background: Atypical myxoma has been reported in various locations in the heart, however, myxoma involving the pulmonary valve is rare. Here we present a case of pulmonic valve myxoma which was resected via a percutaneous approach.
Case Report: A 66-year-old female with known metastatic adenocarcinoma of the lung, and chronic obstructive pulmonary disease presented with acute onset shortness of breath for two days. The patient experienced respiratory arrest en-route to the hospital and required intubation. Computed tomography angiography (CTA) of the chest revealed a new 1.4 x 1.6 cm intracardiac mass along the pulmonary valve. Further evaluation with cardiac magnetic resonance imaging revealed it to be a large vascular tumor on the ventricular side of the pulmonary valve, attached with a narrow stalk. Due to high surgical risk, the patient underwent transesophageal echocardiographic guided percutaneous removal of the mass. Pathology confirmed the mass to be a myxoma.
Conclusion: Atypical myxoma should be considered in the differential diagnosis of valvular masses. Percutaneous resection of valvular masses may be feasible in high-risk surgical patients.

|
Views: 288
HTML: 14
PDF: 140
|
Background: Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease, characterised by multi-organ affections. Haematological involvement is a common manifestation of SLE, consisting of autoimmune peripheral cytopenia. Autoimmune myelofibrosis (AIMF) is a rare cause of cytopenia in SLE; it could precede or be concurrent with the diagnosis of SLE. There are few studies that describe this association.
Case description: We report a case of AIMF revealing the diagnosis of SLE in a 34-year-old female, presented with episodes of gingival bleeding associated with peripheral inflammatory polyarthralgia, photosensitivity and deterioration of general condition. Clinical examination revealed a soft pitting oedema in the lower limbs. Laboratory investigations showed a pancytopenia, inflammatory biological syndrome, with positive 24-hour proteinuria and anti-native DNA antibodies. A bone marrow biopsy showed diffuse myelofibrosis associated with maturation disorders and no tumour infiltrate. Renal biopsy revealed proliferative glomerulonephritis class III with immune deposits.
Conclusion: The association of AIMF with SLE has been rarely reported, and it could be another cause for cytopenia in SLE.

|
Views: 199
HTML: 11
PDF: 124
|
Syncope is a brief loss of consciousness caused by reduced blood flow to the brain, characterised by sudden onset, short duration and full recovery without intervention. Anamnesis, physical examination and other diagnostic tests such as laboratory analysis and electrocardiogram (ECG) can be conducted to identify the underlying cause of syncope. A Brugada pattern on an ECG in individuals with syndrome of inappropriate antidiuretic hormone secretion (SIADH) who have syncope symptoms may indicate cardiac issues. A 69-year-old man with hypertension and a history of smoking presented with syncope. His vital signs were within normal limits, with no signs of a neurological deficit. The patient met the diagnostic criteria for SIADH, as evidenced by the presence of hyponatraemia (Na 118 mmol/l), a hyperosmolar condition and euvolemia. Upon arrival, a twelve-lead ECG showed ST-segment anomalies that reflected a Brugada ECG pattern. No ventricular arrhythmias were detected during the 24-hour Holter monitoring. Coronary angiography revealed no abnormalities in the coronary arteries. The ECG demonstrated the normalisation of ST elevations and the disappearance of the Brugada ECG pattern after the correction of hyponatraemia. After three months of follow-up the patient, with a normal sodium level, had no episodes of syncope.

|
Views: 216
HTML: 11
PDF: 126
|
Introduction: Diffuse large B-cell lymphoma (DLBCL) is a prevalent subtype of non-Hodgkin lymphoma (NHL) affecting predominantly elderly individuals.
Case description: A 68-year-old man with a history of hypertension, hyperlipidaemia and a small pituitary gland tumour presented with sudden-onset binocular diplopia and right-eye blurry vision. A magnetic resonance imaging (MRI) of the brain revealed enhancing soft tissue in the right superolateral orbit inseparable from the lacrimal gland, extending medially to the right superior rectus muscle and soft tissue. Further scanning showed widespread metastasis to the bilateral retroperitoneal lymph nodes, adrenal gland, spine and lymph nodes in the neck. A biopsy of the lacrimal gland confirmed DLBCL.
Conclusion: Primary lacrimal gland DLBCL is a rare and delayed diagnosis that often stems from the resemblance of its clinical manifestations to more benign conditions such as dacryocystitis, dacryostenosis or mucocele. Timely recognition and accurate diagnosis are essential for initiating appropriate treatment and improving patient outcomes.
|
Views: 185
HTML: 15
PDF: 132
|
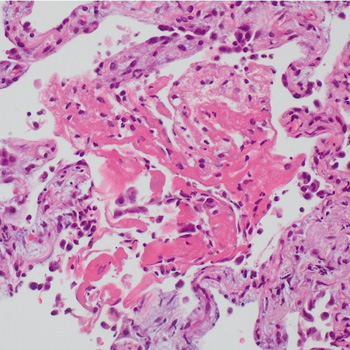
A patient initially treated with corticosteroids for cryptogenic organising pneumonia following pulmonary infarction, developed a worsening condition with progressive cavitary formations in both lower lung lobes. Contrast-enhanced chest computed tomography revealed a pulmonary embolism, and serum anti-Aspergillus IgG antibody analysis yielded a strong positive result. Consequently, the patient was diagnosed with pulmonary infarction with Aspergillus infection; organising pneumonia in surrounding areas reflected the repair process. Following treatment with anticoagulants and antifungal agents, the patient was successfully discharged. Hence, pulmonary infarction should be considered in cases of refractory lung lesions.
|
Views: 244
HTML: 9
PDF: 169
|
Background: Fournier’s gangrene represents a life-threatening necrotising infection affecting the perineal region, while hidradenitis suppurativa is characterised by a chronic inflammatory skin condition. The simultaneous occurrence of both conditions is exceedingly rare.
Case description: A 42-year-old female with a documented history of severe untreated hidradenitis suppurativa presented for shortness of breath, fever and lethargy, along with extensive wounds and skin breakdown involving the left axilla, perineum, lower back, lumbosacral region and bilateral gluteal areas, extending to the perineum. Upon presentation, the patient was in a state of septic shock, and a diagnosis of actively manifesting Fournier’s gangrene was established at the site of the pre-existing hidradenitis suppurativa lesions. Despite the implementation of an aggressive multidisciplinary approach incorporating surgical interventions, antibiotic therapy and intensive care measures, the patient’s condition deteriorated, culminating in septic shock, multi-organ failure and eventual demise. In this report, we discuss both clinical entities, their similarities and differences, and the possible mechanisms by which they may have co-occurred.
Conclusion: The co-existence of hidradenitis suppurativa and Fournier’s gangrene poses unique challenges, given the rapid progression of Fournier’s gangrene within the context of hidradenitis suppurativa, potentially suggesting the latter as a predisposing factor. This case underscores the importance of vigilant screening and management of hidradenitis suppurativa.

|
Views: 152
HTML: 21
PDF: 83
|
Positron emission tomography (PET) has gained widespread acceptance as a valuable diagnostic tool for cancer. It is rare for a PET/CT scan to overlook the presence of metastatic disease. Sebaceous carcinoma is an uncommon malignant tumour that typically originates in the skin of the eyelid. In this case report, we present a unique case involving a metastatic sebaceous carcinoma that was not initially detected by a PET/CT scan in an 88-year-old female. Therefore, clinicians must maintain a heightened awareness of sebaceous carcinoma and exercise caution when making decisions solely based on PET scan results. It is crucial to recognise this potential limitation of PET scans in sebaceous carcinoma and consider further diagnostic approaches to ensure timely and accurate detection of sebaceous carcinoma.

|
A rare case of biloma after ascending cholangitis and endoscopic retrograde cholangiopancreatography
Views: 238
HTML: 29
PDF: 139
|
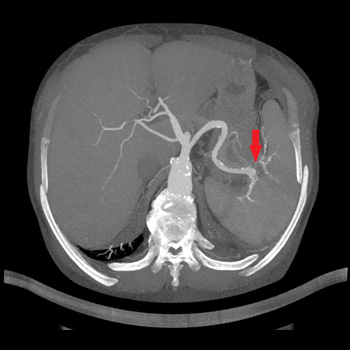
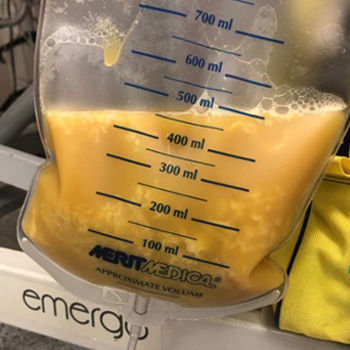
Introduction: Biloma is an uncommon form of liver abscess composed of bile usually associated with procedures of the biliary tree and gallbladder. Cholangitis can be acute or chronic, can result in partial or complete obstruction of the flow of bile. The infection of the bile is so common, that positive blood cultures are highly characteristic. In the case of a suppurative cholangitis with signs of sepsis treatment alone with antibiotics is usually not sufficient to achieve medical remission. Multiple hepatic abscesses are often present, and the mortality approaches 100% unless prompt endoscopic or surgical relief of the obstruction and drainage of infected bile are carried out. Endoscopic retrograde cholangiopancreatography ERCP with endoscopic sphincterotomy is the preferred initial procedure for both establishing a definitive diagnosis and providing effective therapy.
Case description: We present the case of a 69-year-old female patient with complex chronic comorbidities who presented with acute cholangitis initially managed with endoscopically inserted stent and later complicated by sepsis and biloma formation. The bile was drained, and it showed an infection with Candida spp. requiring antifungal therapy.
Conclusions: The failure to perform sphincterotomy in patients with suppurative cholangitis can contribute to the backflow of bile and worse outcomes.
|
Views: 222
HTML: 18
PDF: 161
|
Background: Small cell lung cancer is an aggressive tumor with a poor prognosis that requires prompt treatment. While radiotherapy may enhance survival when superior vena cava syndrome is present, radiation therapy–induced pericardial disease can be a potential complication.
Case Report: A 55-year-old man, who recently underwent radiotherapy for stage IV small-cell lung cancer complicated by superior vena cava syndrome, presented with chest pain and dyspnea. In the emergency room, he was dyspneic, hypotensive, and tachycardic. Pulmonary auscultation revealed the absence of lung sounds on the right. The initial electrocardiogram showed ST-segment elevation in lateral leads and in lead DII, with reciprocal changes in lead DIII. A bedside transthoracic echocardiogram revealed cardiac tamponade and emergent pericardiocentesis was performed, removing 500 ml of purulent fluid, resulting in an immediate clinical improvement. Thoracentesis was also performed, showing no empyema. Large spectrum empirical antibiotic therapy was started. Cultures from the pericardial fluid and peripheral blood grew multi-sensitive Streptococcus pneumoniae. Cytological analysis of the pericardial fluid was consistent with infection. The patient improved after 2 weeks of targeted antibiotic therapy and underwent the first cycle of chemotherapy. He was discharged with an early scheduled pulmonology appointment.
Conclusions: Although the most common causes of pericardial effusion in lung cancer are malignant, non-malignant etiologies should also be considered. This patient had an infectious pericardial effusion most probably due to a pericardial-mediastinal mass fistula caused by radiotherapy. This was a diagnostic challenge, both in the emergency room as well in the inpatient setting.

|
Views: 156
HTML: 10
PDF: 126
|
Hamman syndrome is defined as dissection of air in mediastinum and skin fascia usually due to increased intrathoracic pressure. The air leak tends to make its way into pleural and pericardial layers; however, in rare instances air can also dissect into epidural spaces, regarded as pneumorrhachis. We present a case of a young male with a history of polysubstance abuse and e-vaping, who presented with symptoms of altered mental status. Given the concerning physical examination, a computed tomography of the chest was undertaken, which showed pneumothorax, pneumomediastinum and pneumorrhachis. The patient was closely monitored in the intensive care unit and improved after symptomatic management. The symptoms of pneumorrhachis depend on the volume and location of air in intracranial and intraspinal space. Although asymptomatic in our case, it is crucial for clinicians to be aware that pneumorrhachis with Hamman syndrome can potentially cause neurological deficits and cardiopulmonary arrest in severe cases due to increased intraspinal and intracranial hypertension, emphasising the need for close monitoring.
|
Views: 352
HTML: 126
PDF: 340
|
Background: Studies have shown major cardiovascular effects associated with ketamine use disorder including dose-dependent negative inotropic effects. Preoperative ketamine use has been linked to ketamine-induced stress cardiomyopathy.
Case presentation: A 28-year-old female with a history of recurrent cystitis and ketamine use disorder (twice weekly for 14 years) presented with bilateral lower extremity oedema and shortness of breath for 3 months. She was tachycardic with a troponin level of 0.07 ng/ml and a B-type natriuretic peptide (BNP) level of 2511 pg/ml. Electrocardiogram showed normal sinus rhythm and transthoracic echocardiography (TTE) showed left ventricular ejection fraction (EF) of 15%, dilated left ventricle, and severe tricuspid and mitral regurgitation. Computed tomography (CT) scan of the chest and abdomen showed bilateral pleural effusions with congestive hepatopathy and ascites. The patient was started on intravenous furosemide, metoprolol, and sacubitril/valsartan. Rheumatological workup including complement levels, and antinuclear anti-double-stranded DNA was negative. A repeat TTE 2 weeks later revealed an EF of 25% and moderate tricuspid regurgitation. Four months later, the EF was 54% with normal left ventricular cavity size.
Conclusion: Although ketamine use disorder is increasing, data on long-term side effects is minimal. Screening for ketamine use disorders should be considered in patients presenting with acute systolic heart failure. Long-term studies are needed to evaluate the benefits of adding ketamine screening to standard urine toxicology.

|
Views: 274
HTML: 20
PDF: 204
|
Background: Cardiac sarcoidosis can cause a wide range of symptoms, including shortness of breath, chest pain, oedema, and fatal arrhythmias such as ventricular tachycardia (VT). Because the symptoms can be nonspecific, diagnosing cardiac sarcoidosis can be challenging. Treatment options may include corticosteroids to reduce inflammation, immunosuppressive drugs to prevent further damage, medications to control symptoms, ablation procedures, and defibrillators to prevent cardiac arrest.
Case: A 60-year-old woman who has sarcoidosis affecting multiple organs including cardiac sarcoidosis, non-ischemic cardiomyopathy with reduced ejection fraction, and hypertension, was admitted with tachycardia, shortness of breath, and a recently fired automatic implantable cardioverter defibrillator (AICD). Three months prior, the patient was admitted for a syncopal episode and diagnosed with cardiac sarcoidosis through cardiac magnetic resonance imaging (MRI) and positron emission tomography (PET), which demonstrated active inflammation, and an AICD was implanted. During this admission, the patient had an episode of ventricular tachycardia and was treated with amiodarone and lidocaine. The patient received steroids, sacubitril/valsartan, and methotrexate. After 48 hours of observation, the patient was discharged without further events.
Conclusion: Cardiac sarcoidosis is a rare but serious disease that can lead to life-threatening cardiac complications such as ventricular tachycardia. Early diagnosis and aggressive management are crucial for improving outcomes and preventing sudden cardiac death. AICD implantation as a secondary prevention in cardiac sarcoidosis might prevent cardiac arrest.

|
Views: 236
HTML: 13
PDF: 146
|
Introduction: Fever of unknown origin (FUO) refers to a condition of prolonged increased body temperature, without identified causes. The most common cause of FUO worldwide are infections; arthropod bites (loxoscelism) should be considered in view of the spread of the fiddleback spider. Loxoscelism can present in a cutaneous form (a necrotic cutaneous ulcer) or in a systemic form with fever, haemolytic anaemia, rhabdomyolysis and, rarely, macrophage activation syndrome (MAS). For this suspicion, it is important to have actually seen the spider.
Case description: A 71-year-old man was admitted to our department because of intermittent fever, arthralgia and a necrotic skin lesion on his right forearm that appeared after gardening. Laboratory tests were negative for infectious diseases, and several courses of antibiotics were administered empirically without clinical benefit. Whole-body computed tomography showed multiple colliquative lymphadenomegalies, the largest one in the right axilla, presumably of reactive significance. A shave biopsy of the necrotic lesion was performed: culture tests were negative and histological examination showed non-specific necrotic material, so a second skin and lymph node biopsy was performed. The patient developed MAS for which he received corticosteroid therapy with clinical/laboratory benefit. Cutaneous and systemic loxoscelism complicated by MAS was diagnosed. Subsequently, the second biopsy revealed morphological and immunophenotypic findings consistent with primary cutaneous anaplastic large cell lymphoma (PC-ALCL).
Conclusions: Skin lesions and lymphadenomegalies of unknown origin should always be biopsied. It is very common to get indeterminate results, but this does not justify not repeating the procedure to avoid misdiagnosis.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

