
EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 764
HTML: 85
PDF: 395
|
Introduction: Pericardial effusion is common in the setting of rheumatoid arthritis (RA); however, it is rarely its first manifestation.
Case description: An 82-year-old male presented with abdominal pain, vomiting and fever. Blood analysis revealed elevated systemic inflammatory markers, and an abdominal computed tomography scan revealed non-specific alveolar condensation of the right pulmonary base and pericardial effusion subsequently quantified as medium size by transthoracic echocardiography. A large aetiological panel was requested, with the autoimmunity study revealing high levels of rheumatoid factor (RF) and anti-citrullinated cyclic peptide (anti-CCP) antibodies. Since the patient did not present articular involvement, the initial hypothesis was pericardial effusion due to pneumonia and no specific treatment for RA was started. At follow-up, the pericardial effusion recurred and a pericardiocentesis was performed. The pericardial fluid analysis was sterile, and no malignant cells were identified. A new serological study confirmed high levels of RF and anti-CCP antibodies, and immunomodulatory treatment was initiated. After one year, the pericardial effusion recurred due to non-compliance with immunomodulatory therapy. A surgical pleuro-pericardial window was performed, and the cytological study of the pericardial patch revealed submesothelial thickening and foci of perivascular lymphocytic infiltrate. The patient remained asymptomatic.
Discussion: After exclusion of a large spectrum of infectious and non-infectious causes and the relapse after suspension of immunomodulatory treatment, the most probable aetiology for the pericardial effusion remains RA.
Conclusion: Pericardial syndromes can be the first manifestation of AR even in the absence of articular symptoms and this disease must be considered in the aetiological investigation.

|
Views: 345
HTML: 67
PDF: 275
|
Introduction: Individuals who have had severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection may develop post-coronavirus disease conditions, also known as long COVID. The symptoms of long COVID are nonspecific, and there are similarities between the symptoms of long COVID and those of Graves’ disease (GD). Therefore, it is important to rule out GD in patients suspected of having long COVID. Telemedicine is widely used to avoid the risk of SARS-CoV-2 infection. However, owing to the lack of in-person examinations, diagnostic errors can occur.
Case description: A 27-year-old Japanese woman presented complaining of persistent fatigue, dyspnea, and low-grade fever, and after in-person examination was finally diagnosed with GD. She had been diagnosed with SARS-CoV-2 infection four months earlier and her symptoms had resolved within 5 days but then recurred. Subsequently, she had 3 telemedicine visits and had been diagnosed with long COVID.
Discussion: With telemedicine there may be delayed diagnosis of GD in patients with a recent history of SARS-CoV-2 infection. Some symptoms and abnormalities cannot be confirmed in telemedicine visits performed using a simple mobile phone. Therefore it is important to know which findings obtained in telemedicine visits with a simple mobile phone are suggestive of GD. Low-grade fever and tachycardia are often observed in patients with GD, but rarely occur in patients with long COVID.
Conclusion: Tachycardia and persistent low-grade fever after SARS-CoV-2 infection, which can be confirmed by telemedicine, can be clues for the diagnosis of GD. Therefore, in-person examination should be added if these symptoms are confirmed by telemedicine.
|
Views: 453
HTML: 68
PDF: 354
|
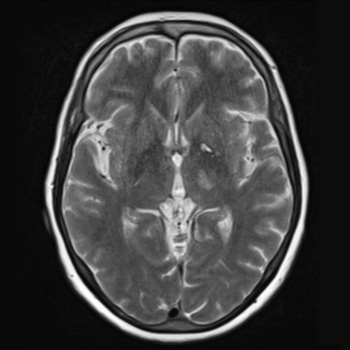
Introduction: Neurosyphilis (NS) refers to a central nervous system infection caused by Treponema pallidum. In recent years, there has been an increasing incidence of syphilis; however, NS is uncommon compared to the era before the discovery of penicillin. Manifestations are usually non-specific, ranging from asymptomatic cases to syphilitic meningitis, meningovascular syphilis, general paresis and tabes dorsalis. Meningovascular syphilis can cause an inflammatory arteritis of cerebral arteries, leading to vascular occlusion and cerebral infarction.
Case description: We report a case of an ischaemic stroke in a patient with several vascular risk factors, presenting with right hemiparesis, hemihypesthesia and dysarthria. Initial computed tomography with angiography of the head and neck was normal; however, magnetic resonance imaging of the brain revealed a thalamic and internal capsule infarct. Serum T. pallidum antibodies were positive, as well as a rapid plasma reagin test. Cerebrospinal fluid analysis confirmed the diagnosis of neurosyphilis, and the patient was treated with ceftriaxone for 14 days due to a penicillin allergy.
Discussion and conclusion: Although there is a high prevalence of stroke in patients with NS, this condition is typically underdiagnosed. Untreated NS carries a higher risk of stroke recurrence compared to other risk factors. Therefore, early diagnosis and treatment are essential. This case highlights the importance of considering NS in stroke victims, even in older patients with several additional vascular risk factors, to prevent recurrence and other complications.
|
Views: 454
HTML: 65
PDF: 372
|
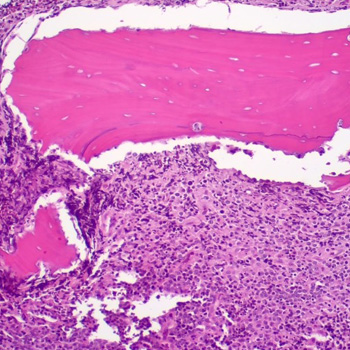
Background: Primary bone lymphoma (PBL) is a rare form of extra nodal non-Hodgkin’s lymphoma (NHL).
Case description: We describe a 39-year-old-male with no medical history who presented with unilateral facial swelling following a tooth extraction. Initial diagnoses after various presentations over the course of three weeks, based on inflammatory and infectious aetiologies. However, the patient was ultimately diagnosed with diffuse large B-cell lymphoma.
Discussion: Symptoms of PBL are very similar to inflammatory and infectious diseases of the bone, such as osteomyelitis or osteonecrosis. Clinical features of PBL involving the head and neck include persistent jaw pain, tooth mobility secondary to extensive destruction of bone, and in advanced cases, lip numbness and swelling. On examination it may present as an exposed necrotic bone with surrounding soft tissue oedema. Misdiagnosis of these lesions as an infectious or inflammatory aetiology may lead to an unnecessary delay in lymphoma treatment, and subsequently worsen the prognosis if caught at a later stage. Therefore, any concerning lesion, especially in the oral cavity, must be subjected to early histopathological evaluation to differentiate PBL from osteomyelitis and/or osteonecrosis.
Conclusion: This case report highlights the importance of an early histopathological evaluation to prevent delay in the diagnosis of primary bone lymphomas.
|
Views: 323
HTML: 52
PDF: 293
|
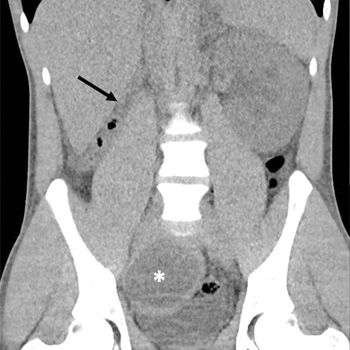
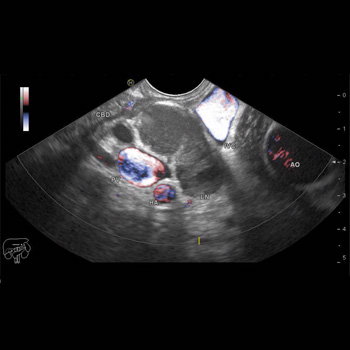
We report the case of a 24-year-old male presenting with obstructive renal failure, characterised by imaging evidence of a cystic lesion contingent upon the seminal vesicle and concurrent renal agenesis. Initial management involved urinary diversion, followed by outpatient monitoring and subsequent recurrence. Subsequent diagnostic assessments led to the identification of Zinner's syndrome, accompanied by retroperitoneal fibrosis. We present the clinical course, diagnostic methodology and the efficacious implementation of medical-surgical therapeutic interventions, yielding favourable outcomes.
|
Views: 433
HTML: 52
PDF: 294
|
Background: Rhodococcus equi is a Gram-positive microorganism that causes infections, particularly in immunocompromised patients. Treatment duration can be prolonged. While vancomycin is an effective drug in this scenario, its use may lead to renal damage. Studies have shown that continuous vancomycin infusion appears to be a safe strategy in terms of adverse effects compared to bolus administration.
Case description: We present the case of a 71-year-old female liver transplant recipient. After being diagnosed with a mediastinal infection caused by Rhodococcus equi with poor response to initial therapy, she required 12 months of continuous intravenous domiciliary infusion of vancomycin combined with oral levofloxacin and rifampicin. There was no drug-related complication throughout the follow-up.
Conclusions: The use of continuous vancomycin infusion has emerged as a safer, more efficient, and cost-effective alternative to intermittent administration. We want to emphasise the uniqueness of this case, where despite the unprecedented treatment duration, no adverse effects occurred.

|
Views: 358
HTML: 60
PDF: 292
|
Background: Transient myoclonic (TM) state in older adults is a neurological condition characterised by short-lived, repetitive myoclonus without consciousness disturbance. First reported in 1992, it predominantly affects older individuals with chronic diseases. Despite its clear symptomatology, TM often remains under-recognised, leading to potential misdiagnoses.
Case description: We report a case of a 68-year-old woman with a history of chronic heart failure who developed TM during hospitalisation following medication adjustment for acute heart failure. The patient, who had no history of intracranial disease or epilepsy, experienced acute involuntary movements of the face and limbs three days after diuretic adjustment. She responded well to intravenous diazepam and oral clonazepam, with no recurrence of symptoms post-treatment.
Discussion: TM presents with bilateral, irregular, and repetitive myoclonus, mostly affecting the head, neck and upper extremities. Diagnosis is clinical, based on symptomatology and normal laboratory results. This case underscores the importance of recognising TM in differential diagnosis, especially in older patients in the acute or recovery phase of infection, or with medication changes. The potential role of fluid volume changes in TM pathophysiology in patients with underlying conditions such as hypertension or chronic heart failure is also highlighted. This case emphasises the need for heightened awareness and knowledge of TM among healthcare professionals.
Conclusions: TM, though rare, requires awareness among clinicians for accurate diagnosis and management. It is crucial to avoid misdiagnosis and unnecessary interventions, and to provide appropriate information during care transitions, particularly in older adults with chronic conditions.
|
Views: 265
HTML: 52
PDF: 230
|
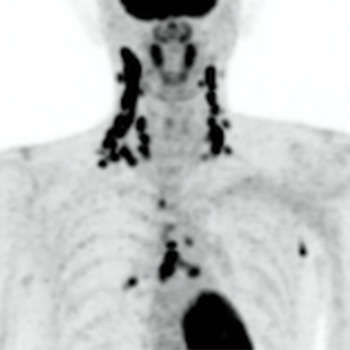
Kikuchi-Fujimoto disease (KFD), also called histiocytic necrotizing lymphadenitis, is more common in young women and typically presents with small, painful, localized cervical lymphadenopathy that resolves spontaneously within a few weeks. Laboratory findings are variable. As many as 40% of KFD cases are reported to be painless, and up to 22% to be generalized lymphadenopathy. Therefore, malignant lymphoma could be a differential diagnosis of KFD. A histopathologic diagnosis is needed when it is difficult to distinguish KFD from lymphoma. KFD typically shows small, highly accumulated cervical lymph nodes on fluorodeoxyglucose positron emission tomography (FDG-PET). This contrasts with malignant lymphoma, which tends to be associated with massive lymphadenopathy. In our case, a 40-year-old Japanese male presented with painless lumps in the right neck, accompanied by fever, night sweats, and loss of appetite. His symptoms and laboratory results worsened over a month. FDG-PET revealed highly accumulated uptake in cervical, mediastinal, and axillary lymph nodes. The PET imaging showed a small, high FDG uptake and contributed to the correct diagnosis of KFD. This case report highlights the importance of FDG-PET, which is a valuable diagnostic tool for KFD as it typically differentiates large clusters of small lymph nodes typical of KFD from normal lymph nodes.
|
Views: 370
HTML: 117
PDF: 313
|
Cytomegalovirus (CMV) infection is often asymptomatic. However, in certain individuals, it can cause non-specific signs and symptoms that maybe hard to recognise. The condition may therefore be overlooked or misdiagnosed, leading to prolonged illness and serious sequelae. In this case report, we present a rare instance of CMV infection in an HIV-negative patient who had a remote history of splenectomy and was experiencing prolonged fever and markedly elevated white blood cell (WBC) count.
|
Views: 556
HTML: 54
PDF: 336
|
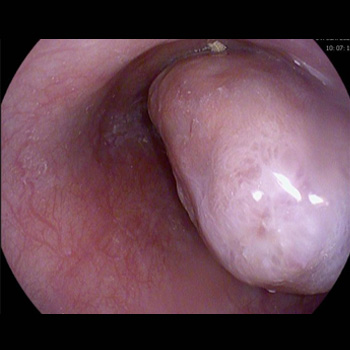
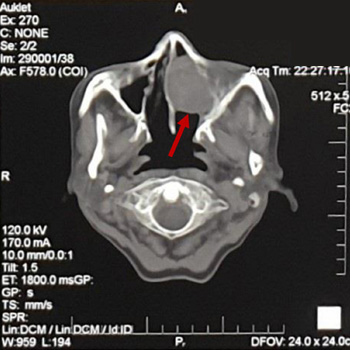
A nuclear protein in testis (NUT) midline carcinoma arises from squamous cells and is often located in the head, neck, and lungs. This report focuses on the negative p63 mutation and older age at the diagnosis of a NUT carcinoma, which has significant prognostic implications. A 62-year-old patient presented initially with a three-year history of recurring frontal headaches, intermittent nasal bleeding, and a sensation of a nasal cavity mass. An incisional biopsy revealed a poorly differentiated NUT carcinoma in the left maxillary sinus. A functional endoscopic sinus surgery was performed, but the cancer recurred. As a result, a total maxillectomy was performed, and the patient was declared cancer-free with no evidence of residual disease. This is a rare instance of a p63-negative midline NUT cell carcinoma (NCC) in an elderly patient, which could potentially contribute to a more favourable prognosis and longer survival compared to other reported cases.

|
Views: 425
PDF: 389
HTML: 92
|
MELAS – an acronym for mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes – is a multiorgan disease caused by a mutation in mitochondrial DNA (mtDNA). Its clinical manifestations are highly variable; mainly stroke-like episodes, seizures, recurrent headaches, or muscle weakness. However, gastrointestinal complications such as chronic intestinal pseudo-obstruction (IPO), pancreatitis, gastroparesis and hepatopathy are also common. In this report we describe a young patient with gastrointestinal complication of MELAS which led to superior mesenteric artery syndrome (SMAS). It is rare but not surprising combination and should be considered in cases with significant weight loss and resistance to symptomatic treatment. The optimal energy support is the main pillar of the treatment.
|
Views: 465
HTML: 55
PDF: 278
|
Tuberculosis (TB) is primarily a respiratory infection with huge mortality and morbidity worldwide. Extrapulmonary TB infection is common, affecting lymph nodes, pleura, and abdomen, but the primary biliary presentation without lung involvement is exceedingly rare. We report on a 38-year-old male patient who presented with isolated obstructive jaundice secondary to TB infection. This case highlights the importance of considering TB infection in the differential diagnosis of obstructive jaundice, especially in the endemic area. We also provide a literature review on TB infection, mainly in the biliary tract.

|
Views: 413
HTML: 113
PDF: 283
|
Background: Beau's lines are transverse grooves in the nail plate that result from transient interruption of the growth of the proximal nail matrix. These rare nail disorders can be triggered mostly by infections or systemic diseases.
Case Description: We describe a 65-year-old man who presented with nail changes on all fingernails. The patient, a non-smoker with no medication history, had severe immune responses during two hospitalisations, 9 and 4 months ago, for COVID-19. Both hospitalisations were accompanied by markedly elevated interleukin-6 levels, and treatment with tocilizumab on top of dexamethasone was required. The present examination revealed Beau's lines which were associated with both prior COVID-19 infections.
Conclusions: Although nail changes look harmless, seeking Beau's lines during the physical examination might indicate past severe COVID-19 infection and a higher probability for reinfection and rehospitalisation.

|
Views: 275
HTML: 77
PDF: 261
|
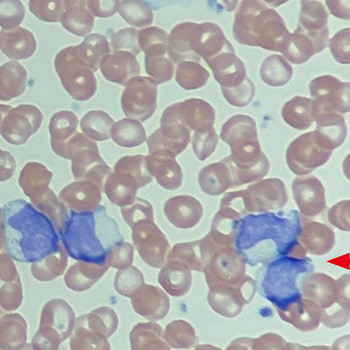
Ertapenem, a carbapenem-type beta-lactam antibiotic, demonstrates broad-spectrum efficacy against a wide range of Gram-positive and Gram-negative bacteria, including aerobes and anaerobes. Importantly, it demonstrates resistance to virtually all beta-lactamases, including the extended spectrum beta-lactamases (ESBLs). Haematologic complications such as thrombocytosis, haemolysis, anaemia, and neutropenia are infrequent side effects associated with this drug. In this report, we present a rare case of ertapenem-induced thrombocytosis in a 62-year-old female patient who was admitted for a complicated urinary tract infection caused by Escherichia coli.

|
Views: 298
HTML: 49
PDF: 282
|
A 52-year-old female with a history of chronic lymphoedema and untreated deep vein thrombosis, presented with non-specific right-sided chest pain. A CT angiogram confirmed bilateral inferior pulmonary vein thromboses (PVT). A comprehensive hypercoagulable workup and age-appropriate cancer screening were unremarkable; the lack of associated risk factors confirmed idiopathic PVT. The management strategy of systemic anticoagulation with apixaban and multidisciplinary follow-up underscores the treatment challenges of rare presentations. This case accentuates the importance of considering PVT in differential diagnoses of atypical chest pain and contributes valuable insights into the diagnosis, understanding and management of this uncommon condition.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

