EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 0
HTML: 0
PDF: 0
|
Tumour-to-tumour metastasis (TTM) is a rare phenomenon that clinicians should be aware of when evaluating patients with a history of prostate cancer. We present the diagnosis and management of an 80-year-old former smoker with high-risk prostate cancer, who developed a lung nodule consistent with TTM. The patient had concurrent primary lung adenocarcinoma and metastatic prostate cancer, making this a unique case of dual primary and metastatic malignancies. The complexity of this case highlights the need for comprehensive evaluation and interdisciplinary management in patients with multiple malignancies. The literature review reveals that these are extremely rare occurrences, with most cases involving metastasis to the second primary tumour. Despite the challenges in diagnosing preoperatively, it is important to consider TTM as a possibility in patients with prostate cancer who present with a lung nodule. This report presents one of the few documented cases of TTM. It also reviews relevant cases in the literature and discusses the current situation in relation to established criteria for classifying combination tumours.

|
Views: 0
HTML: 0
PDF: 0
|
Background: Acute pancreatitis is a common cause of hospitalisation characterised by inflammation of the pancreas. While mechanical, toxic and iatrogenic factors typically cause it, post-oesophagogastroduodenoscopy (EGD) pancreatitis is extremely rare. This report examines a case of acute pancreatitis following EGD, aiming to highlight this rare but significant complication.
Case description: A 46-year-old woman with a history of breast cancer, anxiety, vitamin D deficiency and gastro-oesophageal reflux disease underwent an EGD, which revealed and led to the removal of duodenal polyps. Six hours post-procedure, she presented with severe abdominal pain radiating to her back, accompanied by nausea. Laboratory results indicated elevated lipase levels, and a computed tomography (CT) scan confirmed acute pancreatitis. The patient was managed with aggressive fluid resuscitation, bowel rest and pain management, leading to an improvement in her condition and subsequent discharge. We believe that the pancreatitis was likely caused by the use of cautery during the endoscopic mucosal resection of duodenal polyps.
Conclusion: This case underscores the need for clinicians to recognise acute pancreatitis as a potential complication of EGD, especially in the absence of other common risk factors.

|
Views: 24
PDF: 7
HTML: 6
|
Introduction: Renal squamous cell carcinoma (SCC) is a neoplasm with an extremely rare occurrence compared to other renal malignancies. The classic presentation includes a palpable mass and flank pain; however, the presentation is seldom non-specific. Our study describes the significance of programmed death ligand-1 (PD-L1) expression in renal cancer and its association with clinical outcomes, alongside available treatment options.
Case description: An 80-year-old female with a history of hypertension and cerebral aneurysm presented with right flank pain and blood in urine and was diagnosed with pyelonephritis and left renal mass/phlegmon. A biopsy revealed SCC of the kidney with metastasis to the lung and aortocaval lymph node. Positron emission tomography (PET) scan confirmed malignancy in the kidney and lung. Treatment with pemrolizumab and carboplatin plus paclitaxel was initiated but poorly tolerated as the haemoglobin dropped rapidly.
Conclusion: SCC poses a diagnostic challenge due to its rarity and non-specific symptoms, often leading to advanced stage diagnosis. PD-L1 expression is pivotal in assessing tumour aggressiveness and prognosis. PD-L1 inhibitors offer promise, but their efficacy in renal SCC warrants further investigation. Radical nephrectomy and systemic chemotherapy show potential in advanced cases, necessitating vigilant management of treatment-related side effects. This case emphasises the need for ongoing research to refine therapeutic approaches and enhance outcomes in renal SCC patients.

|
Views: 23
HTML: 1
PDF: 8
|
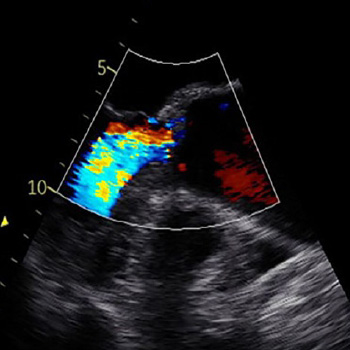
The maze procedure for atrial fibrillation carries risks, including pleural effusion. We report a case of a 54-year-old woman with right-sided pleural effusion post maze surgery, presenting with dyspnoea. Despite treatment, complications arose, including atrial flutter. Prompt recognition and multidisciplinary management led to a favourable outcome. This case underscores the importance of vigilance for rare post-operative complications and highlights the need for collaborative care in optimising patient outcomes following cardiac surgeries. Further research is warranted to refine management strategies for such occurrences.

|
Views: 78
HTML: 28
PDF: 61
|
Romiplostim and eltrombopag are synthetic agonists of the thrombopoietin receptor (TPO-R), commonly used for immune thrombocytopenic purpura (ITP) and sometimes in myelodysplastic syndrome (MDS). They are rarely associated with kidney injury. We report a case of acute kidney injury caused by romiplostim and eltrombopag in an 80-year-old male patient with MDS and ITP. He did not have systemic haemolysis syndrome but isolated acute renal thrombotic microangiopathy confirmed by kidney biopsy. He was treated with steroids, plasmapheresis and anticoagulation, with improvement in renal function. Interestingly, the patient had high antiphospholipid (aPL) antibodies noted upon screening, indicating a possible new antiphospholipid syndrome (APS) diagnosis. In the presence of circulating aPL antibodies, eltrombopag may have served as a trigger, causing endothelial injury and subsequent renal microangiopathy; aPL antibodies were still significantly positive at four weeks of outpatient testing. This case and a few others reported in the literature highlight the importance of screening for aPL antibodies before initiating TPO-R agonists in patients with ITP. We suspect that using TPO-R agonists, rather than underlying aPL, caused renal failure.

|
Views: 113
HTML: 25
PDF: 102
|
Neutropenia by non-chemotherapy drugs is an extremely rare idiosyncratic life-threatening drug reaction. Ceftriaxone and meropenem are widely used broad-spectrum antibiotics and are generally safe and well tolerated. The authors present a case of neutropenia induced by ceftriaxone and meropenem in an adult patient. The resolution of neutropenia occurred within 48 hours of ceftriaxone and meropenem being discontinued. Although antibiotic-induced neutropenia is uncommon, clinicians should be mindful of this adverse drug effect because of its potential development of severe neutropenia, septicaemia, septic shock, deep-seated infections and even death. Therefore, neutropenic sepsis treatment should be initiated without delay, particularly if the patient becomes septic and febrile. Granulocyte-colony stimulation factor (G-CSF) may be administered to facilitate the recovery process with daily monitoring of neutrophil count. Mortalities from antibiotic-induced neutropenia remain rare, with a range of 2.5–5%.

|
Views: 313
HTML: 14
PDF: 171
|
Background: A case of bilateral multifocal serous retinal detachments and dry eye complicated with unilateral peripheral ulcerative keratitis (PUK) during erdafitinib therapy is described.
Case description: A 76-year-old male underwent a baseline examination two months after initiating 8 mg erdafitinib therapy (April 2023) due to metastatic urothelial carcinoma. Left subfoveal serous retinal detachment was observed initially but the treatment was resumed as he was asymptomatic. In May 2023, bilateral multifocal subretinal fluid pockets were identified, and the patient was still asymptomatic. However, in June 2023 he complained of bilateral redness and a stinging sensation in his right eye. Bilateral severe dry eye and right PUK were diagnosed. He was prescribed dexamethasone eye drops and sodium hyaluronate artificial tears for both eyes. One week later corneal staining decreased, and progression of PUK ceased. Erdafitinib therapy was discontinued in June 2023 due to the planned transurethral prostatectomy. By July 2023, after discontinuation of the drug and administration of the topical treatment, the dry eye improved and the PUK became inactive. There was also resolution of subretinal fluid pockets in the right eye and a reduction of subretinal fluid pockets in the left eye. After the reinitiation of erdafitinib therapy, serous retinal detachments recurred in both eyes in September 2023, but both corneas remained stable with topical low-dose dexamethasone, cyclosporine-A and artificial tear usage.
Conclusion: Erdafitinib therapy may lead to concurrent anterior and posterior segment complications. Multidisciplinary monitoring is crucial for patients undergoing erdafitinib therapy to prevent possible visual disturbances.

|
Views: 421
HTML: 24
PDF: 252
|
Euglycemic diabetic ketoacidosis (euDKA) is a rare but severe metabolic complication of diabetes mellitus characterised by elevated anion gap metabolic acidosis despite normal or mildly elevated blood glucose levels. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have emerged as effective antidiabetic medications, yet their use is associated with an increased risk of euDKA, especially when coupled with insulin dose reduction.
We present the case of a 50-year-old male with a 20-year history of diabetes mellitus, initially managed with insulin and metformin, who developed euDKA following the introduction of empagliflozin and sitagliptin alongside a reduction in insulin therapy. Despite normoglycaemia the patient exhibited symptoms of ketoacidosis, including chronic fatigue, polydipsia, and polyuria.
Diagnostic workup revealed metabolic acidosis, elevated inflammatory markers, acute kidney injury and ketonuria. Subsequent specialised laboratory tests confirmed type 1 diabetes mellitus (T1DM) with the presence of anti-glutamic acid decarboxylase (anti-GAD) antibodies and the absence of C-peptide secretion. Management involved fluid therapy, intravenous insulin and glucose administration.
This case underscores the diagnostic challenges of euDKA and emphasises the importance of differentiating between T1DM and T2DM, as management strategies vary significantly. Patient education on insulin therapy and injection techniques is crucial to prevent complications such as improper insulin delivery and dose reduction, which can precipitate euDKA.
In conclusion, clinicians should be vigilant for euDKA in patients on SGLT2 inhibitors, particularly when insulin dose reduction is involved. Comprehensive patient education and accurate differentiation between diabetes types are essential for timely diagnosis and optimal management, thereby reducing the risk of severe complications.
|
Views: 137
PDF: 121
HTML: 14
|
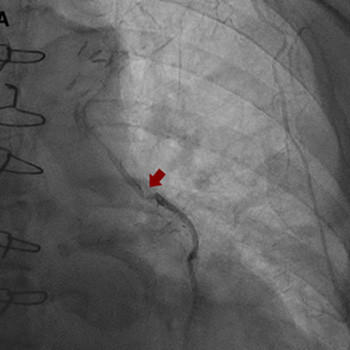
Intracoronary in-stent restenosis (ISR) is a phenomenon that generally occurs between 3 and 6 months after stent placement. With the introduction of drug-eluting stents (DES), the incidence of ISR has decreased but not disappeared. We report a case of reiterant in-stent restenosis of an 81-year-old female patient who underwent multiple percutaneous coronary intervention and two coronary artery bypass surgeries. ISR is possibly associated with extra-stent, stent-related and intra-stent factors. Here, we excluded the first two and focused on the intra-stent factors that seem more likely in our case. A challenging diagnostic workup led us to the hypothesis of a coronary vasculitis potentially triggered by some component of the stent in a predisposed patient carrier of non-disease-specific ANA, with an exaggerated immune response. No recurrence of ISR occurred after the introduction of steroids. Biological and intra-stent causes of ISR should be taken into careful consideration to aim for the early detection of the underlying mechanism of restenosis and to embrace the best therapeutic strategy.
|
Views: 238
HTML: 13
PDF: 219
|
Case description: We describe a case of a patient treated with pembrolizumab (an immune checkpoint inhibitor) for metastatic scalp melanoma. He had a previous history of colorectal cancer, prostatic cancer and chronic polymyalgia rheumatica. The patient was known to have a stable ascending aortic aneurysm of 4.5 cm. However, he developed a rapid expansion of the ascending aortic aneurysm with the size crossing the threshold for surgery. The patient was referred to the cardiothoracic surgery service for intervention and he subsequently underwent surgery. The patient was electively admitted one week later for resection of aortic aneurysm, aortoplasty and external graft fixation. Pathologically, gross evidence of dissection was not identified; however, the histological analysis of the media showed laminar medial necrosis, multifocal in nature, with occasional clusters of histiocytic cells appreciated at their edge reminiscent of that seen in an inflammatory aortitis (granulomatous/giant cell type).
Discussion: Immune checkpoint inhibitor-induced aortitis is becoming increasingly evident, and its presentation can vary. It has been discovered incidentally on surveillance imaging with the use of nivolumab. In other cases, patients have been symptomatic to severely symptomatic. Atezolizumab with carboplatin and etoposide has been reported to cause abdominal aortitis which was responsive to corticosteroids and subsequent discontinuation of atezolizumab. Pembrolizumab has been linked to a case of transverse aortic arch aortitis. In our case, the inflammatory aortitis due to pembrolizumab was the cause of the rapid expansion of the ascending aortic aneurysm.
Conclusion: Patients with known aortic aneurysms should undergo careful surveillance when commencing immune-checkpoint inhibitor therapy.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

