EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 408
HTML: 62
PDF: 361
|
Dasatinib is a tyrosine kinase inhibitor used for treatment of some specific types of leukaemia. The development of pleural effusion is a known adverse effect of dasatinib and chylothorax is exceptional. No case has been reported beyond 5 years of treatment and extensive search for an alternative diagnosis is currently suggested in such scenario. The underlying mechanism is not currently clear. We describe a woman on dasatinib treatment for more than 10 years who developed chylothorax. Drug withdrawal resolved the chylous pleural effusion. We were able to find 14 additional cases of dasatinib-related chylothorax reported up until now.
|
Views: 404
HTML: 71
PDF: 349
|
Tracheoesophageal prosthesis (TEP) is an artificial connection between the trachea and esophagus allowing air into the upper esophagus from the trachea thereby vibrating it. TEPs give patients who lose their vocal cords to laryngectomies a tracheoesophageal voice. A potential complication of this is silent aspiration of gastric content. We present a case of a 69-year-old female with a TEP placed after a laryngectomy for laryngeal cancer who presented to the hospital with shortness of breath and hypoxia. She was initially treated for a presumed diagnosis of chronic obstructive pulmonary disease (COPD) and congestive heart failure (CHF) exacerbations but continued to be hypoxic despite aggressive medical management. Further evaluation revealed silent aspirations as a consequence of TEP malfunction. Through our case report we urge clinicians to consider this differential diagnosis, as the clinical presentation of silent aspiration among patients with a TEP can be easily mistaken for a COPD exacerbation. A large number of patients with TEPs are smokers with underlying COPD.
|
Views: 415
HTML: 78
PDF: 405
|
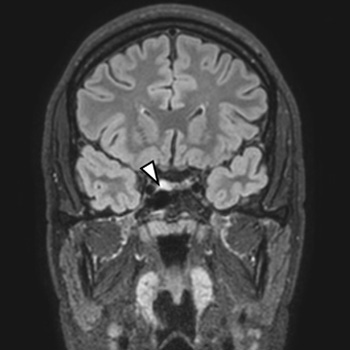
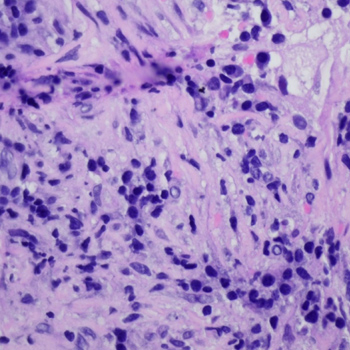
We report a case of a 19-year-old young male presenting with thyrotoxicosis with inappropriately elevated TSH. Magnetic resonance imaging revealed a pituitary adenoma (8.2 x 9.7 mm), TRH stimulation test showed abnormal blunted TSH response, and serum glycoprotein hormone alpha-sub-unit was elevated. He had no family history of thyroid disease and TR-beta genetic testing excluded resistance to thyroid hormone action. The diagnosis of thyrotropin-secreting pituitary adenoma (TSHoma) was presumed and long-acting somatostatin analogue was promptly initiated. After two months of octreotide treatment, serum TSH and FT3 returned to within normal ranges. Tumour resection by transsphenoidal surgery was performed and, ten days after surgery, clinical hypothyroidism was achieved, despite detectable TSH levels (TSH 1.02 µU/ml[RR 0.27-4.2]). Although the patient remained euthyroid for the following three years, there was a gradual biochemical elevation in the levels of TSH, FT4, and FT3 over time, reaching serum values above the normal limit in the third year after surgery. Imaging did not show neoplasm recurrence at this point. After two years, the patient presented with clinical manifestations of re-onset thyrotoxicosis, with MRI revealing a T2 hypersignal oval area compatible with a pituitary adenoma. Adenectomy was performed. Histopathological and immunohistochemical analyses revealed a pituitary adenoma with transcription factor PIT1 expression and positivity for TSH and PRL. TSHoma treatment may not be always effective in the first therapeutic approach and recurrences are a possibility, making follow-up essential. The present case highlights the heterogeneity of post-treatment cure criteria and their limitations.

|
Views: 373
HTML: 72
PDF: 359
|
Primary thyroid lymphoma (PTL) is a rare malignancy of the thyroid gland which should be considered in patients with a rapidly growing cervical mass, especially in those with a history of Hashimoto’s thyroiditis. We present the case of a 53-year-old woman with a rapidly growing goitre with compressive symptoms. Computed tomography (CT) imaging was performed to examine the extent of disease and a biopsy showed B-cell non-Hodgkin lymphoma, stage I according to the Ann Arbor classification. The patient was immediately treated with high-dose prednisone for her compressive symptoms and after the diagnosis she received six cycles of R-CHOP (rituximab-cyclophosphamide-doxorubicin-vincristine-prednisone) chemotherapy. The patient has now been in remission for 12 months. We present this case to demonstrate the importance of awareness of PTL. Up to 10% of cases can be missed with fine needle aspiration cytology (FNAC), making it important to obtain a histological biopsy in rapidly growing goitres. In addition, establishing the correct diagnosis can in most cases prevent unnecessary surgical intervention. The preferred treatment with the best overall survival is chemotherapy with or without radiation therapy.
|
Views: 395
HTML: 118
PDF: 396
|
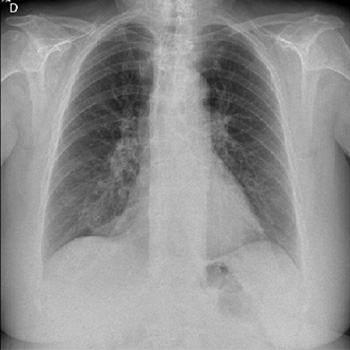
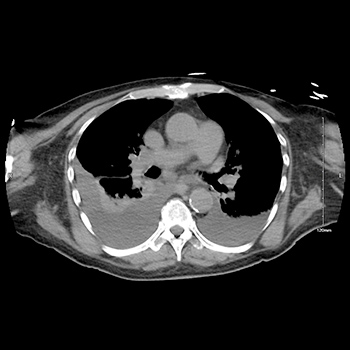
Introduction: Inflammatory myofibroblastic tumours are rare neoplasms which most commonly affect children and young adults. With an intermediate malignant potential, they are typically detected in the abdomen, lung, mediastinum, head and neck, gastrointestinal tract, and genitourinary tract.
Case description: We describe the case of a 33-year-old postpartum woman incidentally diagnosed with a pulmonary inflammatory myofibroblastic tumour following complaints of poorly controlled hypertension a week after caesarean section. She was ALK-negative and received an ALK inhibitor with complete resolution of the lesion. A ROS1–TFG fusion confirmed the diagnosis of an inflammatory myofibroblastic tumour after CT-guided fine needle aspiration.
Discussion: This case highlights an uncommon presentation posing a diagnostic and therapeutic challenge and the potential treatment option of crizotinib.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

