EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 357
HTML: 16
PDF: 290
|
Giant cell arteritis (GCA) may manifest with aggressive intracranial stenosis resistant to medical therapy, and patients may develop refractory neurologic deficits and cerebral infarcts, making GCA a life-threatening condition.
We report the case of a 68-year-old woman recently diagnosed with GCA, medicated with prednisolone 60 mg daily. Two weeks later, the patient was admitted to our Stroke Unit after a sudden episode of global aphasia. Magnetic resonance angiography showed two recent ischaemic lesions, besides an erythrocyte sedimentation rate of 17 mm/hour. A cerebral angiography revealed bilateral stenosis and dilation in the petrous, cavernous and supraclinoid segments of internal carotid arteries (ICA). The patient was started on intravenous methylprednisolone pulses (250 mg daily for five days). Computed tomography (CT) angiography and Doppler ultrasound showed severe vascular disease affecting multiple territories, without significant intracranial involvement. The hypothesis of GCA with extracranial vasculitic involvement was considered as the aetiology of ischaemic cerebral infarctions in multiple territories and, given the severity of the disease, it was decided to add tocilizumab. Despite this, the patient evolved with significant worsening neurological deficits and a CT scan confirmed the presence of new vascular events. Endovascular treatment (EVT) with balloon angioplasty was conducted on both ICAs, with improved calibre and downstream filling. After that, the patient presented sustained clinical improvement, without recurrence of any ischaemic events at the one-year follow-up.
This clinical case stands out for the importance of EVT as an effective therapy in patients with medically refractory GCA with symptomatic intracranial stenosis, improving their prognosis.
|
Views: 435
HTML: 61
PDF: 332
|
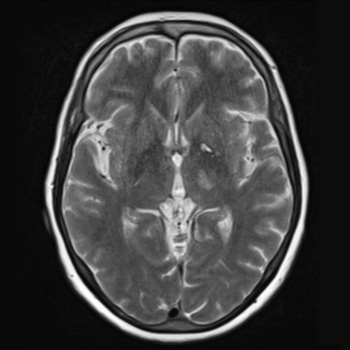
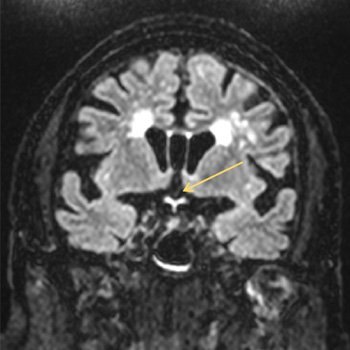
Introduction: Neurosyphilis (NS) refers to a central nervous system infection caused by Treponema pallidum. In recent years, there has been an increasing incidence of syphilis; however, NS is uncommon compared to the era before the discovery of penicillin. Manifestations are usually non-specific, ranging from asymptomatic cases to syphilitic meningitis, meningovascular syphilis, general paresis and tabes dorsalis. Meningovascular syphilis can cause an inflammatory arteritis of cerebral arteries, leading to vascular occlusion and cerebral infarction.
Case description: We report a case of an ischaemic stroke in a patient with several vascular risk factors, presenting with right hemiparesis, hemihypesthesia and dysarthria. Initial computed tomography with angiography of the head and neck was normal; however, magnetic resonance imaging of the brain revealed a thalamic and internal capsule infarct. Serum T. pallidum antibodies were positive, as well as a rapid plasma reagin test. Cerebrospinal fluid analysis confirmed the diagnosis of neurosyphilis, and the patient was treated with ceftriaxone for 14 days due to a penicillin allergy.
Discussion and conclusion: Although there is a high prevalence of stroke in patients with NS, this condition is typically underdiagnosed. Untreated NS carries a higher risk of stroke recurrence compared to other risk factors. Therefore, early diagnosis and treatment are essential. This case highlights the importance of considering NS in stroke victims, even in older patients with several additional vascular risk factors, to prevent recurrence and other complications.
|
Views: 257
HTML: 15
PDF: 223
|
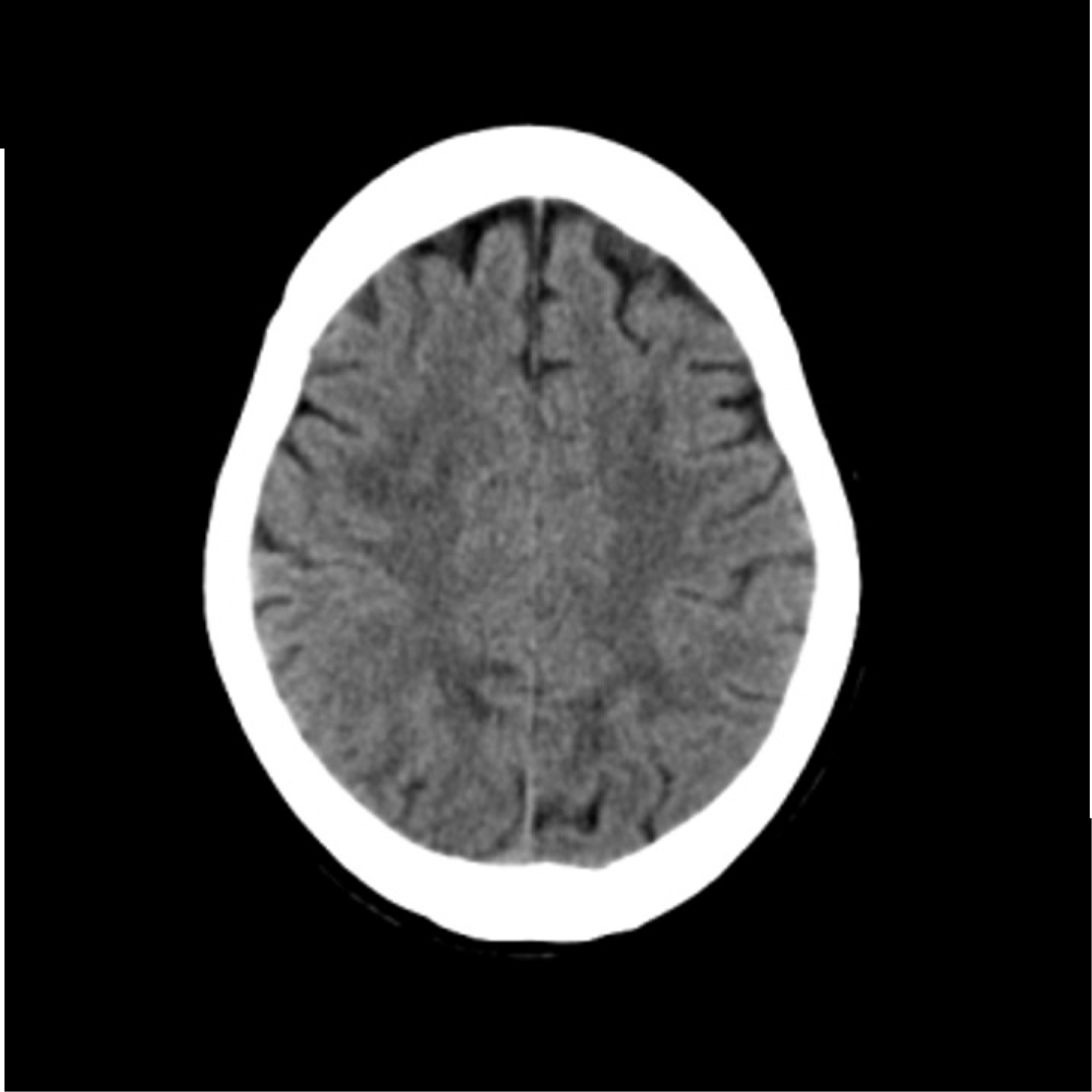
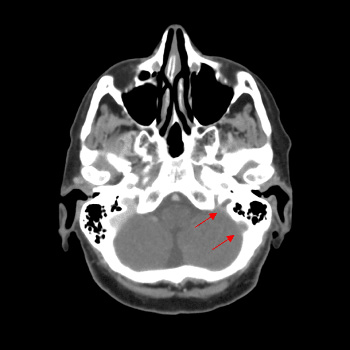
Acute bilateral blindness is an emergent condition that may signal life-threatening disease. The approach focuses on identification of life-threatening disease processes, while differentiating between ocular, psychogenic and neurologic aetiologies. We present the case of an 88-year-old man with multiple cardiovascular risk factors and bilateral chronic glaucoma and cataracts. He presented to the emergency department with sudden onset bilateral loss of visual acuity with no other relevant changes on physical examination, including other neurologic deficits. Ophthalmologic observation showed no sign of acute disease.
Contrast orbit and cranioencephalic CT was unremarkable, so the patient underwent an orbit and cranioencephalic MRI that showed changes in fluid-attenuated inversion recovery (FLAIR) sequences and diffusion restriction involving the optic chiasm and the initial segment of the optic radiations bilaterally. Optic chiasm strokes are rare, owing to the rich supply of collateral circulation. The most frequent presentation is bitemporal hemianopsia but rarer presentations are described. Bilateral loss of visual acuity is very rare and infarction of the whole optic chiasm is unusual.

|
Views: 326
HTML: 88
PDF: 251
|
Introduction: Guillain-Barré syndrome is an acute, inflammatory polyradiculoneuropathy of autoimmune aetiology. It is a rare disease seen in 1 in 100,000 person-years. Up to 20% of those affected develop severe disability; mortality in Guillain-Barré syndrome is 5%. Guillain-Barré, associated with many malignancies as a paraneoplastic phenomenon, has been reported – especially in haematological malignancies such as lymphoma and leukaemia. Solid tumours associated with paraneoplastic Guillain-Barré syndrome are breast and lung cancers. The association between paraneoplastic Guillain-Barré syndrome and gynaecological malignancies are rare, and only a handful of cases have been previously reported in gynaecological cancers.
Case description: We discuss a 65-year-old Sri Lankan female patient diagnosed with metastatic endometrial carcinoma who presented with paraneoplastic Guillain-Barré syndrome. The patient was treated appropriately and eventually recovered from her condition.
Conclusion: Paraneoplastic Guillain-Barré syndrome is a rare phenomenon that clinicians can easily miss, and it has rarely been described in gynaecological cancers. Our patient was diagnosed with this rare phenomenon. The timely recognition and prompt treatment of this potentially life-threatening condition with multiple complications is essential in managing patients with malignancies and neuropathy. Further studies on paraneoplastic Guillain-Barré syndrome are needed as cases may be underreported.

|
Views: 238
HTML: 25
PDF: 215
|
Pituitary apoplexy is an uncommon condition typically resulting from a sudden haemorrhage within a pituitary adenoma. This bleed can present clinically with a wide array of signs and symptoms. This report documents the case of a 62-year-old male who presented to the Lebanese Hospital Geitaoui University Medical Center with signs and symptoms of meningeal irritation. He was initially thought to have meningitis, and was started on antibiotics; he was then found to have pituitary adenoma apoplexy that was complicated by syndrome of inappropriate antidiuretic hormone release (SIADH). The patient was successfully treated with antibiotics, and fluid restriction and hypertonic saline after ruling out other more common causes for his hyponatraemia, before undergoing a transsphenoidal resection of the pituitary adenoma. A three-month follow-up evaluation of the patient demonstrated the absence of hormonal imbalances and the absence of residual tumours on imaging.
|
Views: 347
HTML: 42
PDF: 313
|
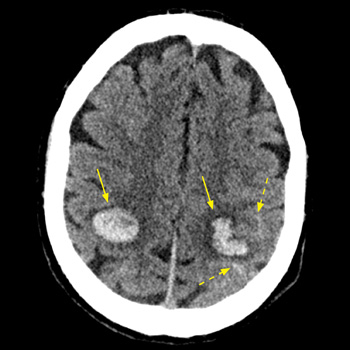
Introduction: Intracranial haemorrhage may complicate infective endocarditis, caused by ruptured mycotic aneurysms or haemorrhagic transformation of brain septic emboli. The risk of intracranial bleeding may increase with the use of non-steroidal anti-inflammatory agent (NSAIDs).
Case description: We report on a 53-year-old male patient with a past history of intravenous drug abuse, who was treated with diclofenac (75 mg IM) for a few hours of preceding fever and arthralgia. Seven hours later he was hospitalised with impaired consciousness and hemiparesis. Evaluation revealed multiple intracranial haemorrhages, at least one originating from a mycotic aneurysm. Repeated blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA), and echocardiography revealed a vegetation on the mitral valve, establishing the diagnosis of bacterial endocarditis.
Conclusion: The abrupt simultaneous multifocal intracranial bleeds shortly following the administration of NSAIDs for a few hours of febrile disease, one clearly originating from a mycotic aneurism, are exceptional. This raises a possibility of a role for diclofenac the intracranial bleeding diathesis in this unique clinical presentation. Intracranial haemorrhage in the set-up of undiagnosed infective endocarditis (IE) might be added to the long list of potential adverse outcomes of NSAID administration, and the possibility of IE should be considered before their administration for febrile disease of undetermined cause.
|
Views: 434
HTML: 92
PDF: 413
|
Introduction: Guillain-Barré syndrome is an immune-mediated inflammatory polyneuritis characterised by rapidly progressive flaccid paralysis. Guillain-Barré syndrome may present with posterior reversible encephalopathy syndrome or reversible cerebral vasoconstriction syndrome in rare cases.
Case description: A woman in her 60s with a history of follicular lymphoma presented with a one-week history of difficulty walking and thunderclap headaches. The patient was diagnosed with Guillain-Barré syndrome based on neurological examination, cerebrospinal fluid analysis and nerve conduction findings. Further diagnosis of posterior reversible encephalopathy and reversible cerebral vasoconstriction syndromes was based on imaging findings and headache history. The patient was treated with intravenous immunoglobulin and amlodipine, and symptoms improved.
Discussion: We reviewed the literature on Guillain-Barré syndrome associated with posterior reversible encephalopathy and/or reversible cerebral vasoconstriction syndrome. The underlying pathophysiology may involve dysautonomia resulting in unstable blood pressure, and hyponatraemia causing endothelial dysfunction. The SNOOP mnemonic highlights the ‘red flags’. This SNOOP mnemonic suggests the possibility of secondary headaches that require imaging studies. In this case, the patient exhibited three SNOOP symptoms: S (history of malignancy: follicular lymphoma), O (sudden-onset headache) and O (over 50 years old).
Conclusion: This case highlights the importance of considering coexisting central neurological disorders in patients with Guillain-Barré syndrome.
|
Views: 350
HTML: 48
PDF: 330
|
Central nervous system (CNS) lymphoma is a rare and aggressive primary neoplasm that comprises a small proportion of brain tumours and non-Hodgkin lymphomas. We present a case report of a 64-year-old woman with CNS lymphoma, who exhibited cognitive changes, weight loss and neurological symptoms. Imaging scans revealed multiple lesions in the brain and thrombosis in the venous sinuses. A diagnosis of diffuse large B-cell lymphoma of the CNS was confirmed through histological examination. The patient underwent treatment with corticosteroids and chemotherapy, but experienced clinical deterioration with thrombocytopenia and disease progression. Despite efforts to manage complications and provide targeted therapy, the patient passed away. Primary CNS lymphoma typically responds well to chemotherapy, and prognostic factors such as age and functional status play a significant role in patient outcomes. However, complications such as thromboembolism pose challenges during treatment due to the hypercoagulable state induced by chemotherapy agents. The pathophysiology of thromboembolic events in the context of malignancy remains uncertain but may involve direct tumour compression, vascular invasion and alterations in coagulation factors. The diagnostic process for CNS lymphoma can be complex, and the information obtained from cerebrospinal fluid analysis, including flow cytometry, may be limited in cases with low cell counts. Ongoing research exploring genetic tests and biomarkers shows promise for improving diagnostic accuracy in such cases. This case underscores the need for comprehensive management strategies that address both the neoplasm and its associated complications, to optimise patient outcomes.

|
Views: 288
PDF: 311
HTML: 87
|
Spontaneous periodic hypothermia (SPH) is an exceptionally rare condition characterised by paroxysmal episodes of spontaneous hypothermia. While commonly associated with Shapiro syndrome, which includes SPH, hyperhidrosis and agenesis of the corpus callosum, there are also cases of SPH that do not exhibit these defining characteristics, known as ‘Shapiro syndrome variant'. These variants may present with diverse brain imaging findings but no agenesis of the corpus callosum, suggesting different potential aetiologies. Notably, the association of SPH with epilepsy has only been reported in a few cases, and confirming epileptic activity in the context of SPH remains a challenge.
In line with this, our report presents two exceptional cases of SPH without significant brain malformation, where we successfully confirmed the presence of epilepsy. The confirmation of epilepsy in these cases is particularly noteworthy, as it adds to the limited documentation of SPH cases with confirmed epilepsy. These findings contribute valuable insights into the association between SPH and epilepsy, enhancing our understanding of this rare condition.
Our report also addresses the broader clinical presentations and the physiopathological mechanisms of SPH. By providing comprehensive insights into these aspects, we aim to advance the existing literature and improve our understanding of SPH and its association with epilepsy.
|
Views: 535
HTML: 119
PDF: 388
|
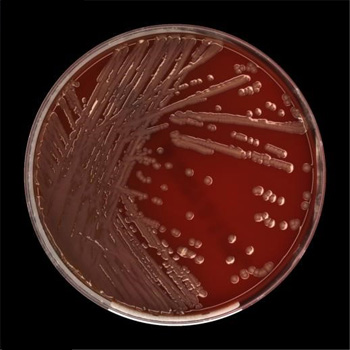
Purpose: Flavobacterium lindanitolerans is an environmental Gram-negative, non-spore-forming rod which is usually not considered to be a human pathogen. Isolation from human clinical samples has been described only once. We report the first case of meningoencephalitis and bacteraemia with Flavobacterium lindanitolerans.
Case description: A 76-year-old female presented with fever, headache, alteration of mental status, marked meningism and dysarthria. A lumbar puncture demonstrated cerebrospinal fluid findings consistent with bacterial meningitis, and a broad-spectrum antibiotic therapy was initiated. Blood and cerebrospinal fluid cultures revealed a growth of Flavobacterium lindanitolerans. Based on antimicrobial susceptibilities testing, antibiotic treatment was changed to levofloxacin, resulting in a remission of the clinical symptoms after 21 days of treatment.
Conclusion: Flavobacterium species are extremely rare human pathogens. However, some of them have been reported to cause opportunistic infections. We describe the first case of meningoencephalitis and bacteraemia caused by Flavobacterium lindanitolerans which was effectively treated with levofloxacin for 21 days.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

