EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 369
HTML: 46
PDF: 248
|
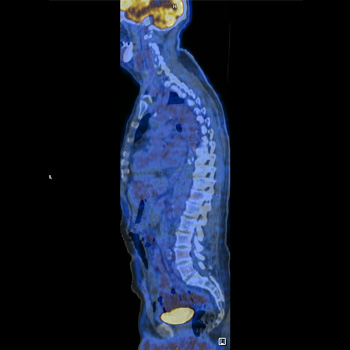
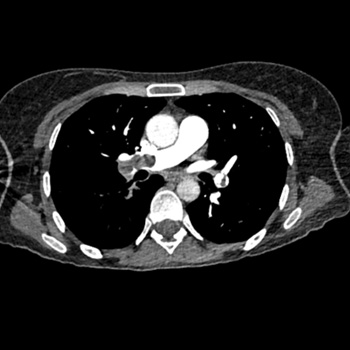
Q fever is a zoonotic infection caused by the pathogen Coxiella burnetii, and patients can present with a wide spectrum of clinical manifestations, depending on whether it is an acute or a chronic infection.
We present the case of a 61-year-old male with fatigue, posterior thoracalgia, intermittent fever, night sweats and weight loss for a month. After an extensive workup, he was diagnosed with acute Q fever with large-vessel vasculitis. The FDG-PET/CT scan suggested an active vasculitis specifically in the thoracic aorta, proximal abdominal aorta, subclavian and carotid vessels, suggesting an immunologic response to acute Q fever infection, barely reported worldwide.
|
Views: 305
HTML: 27
PDF: 269
|
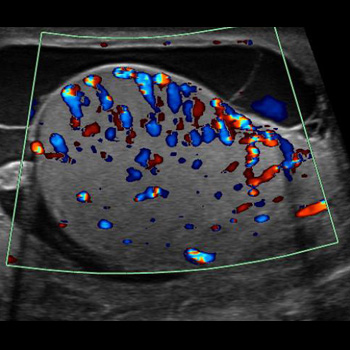
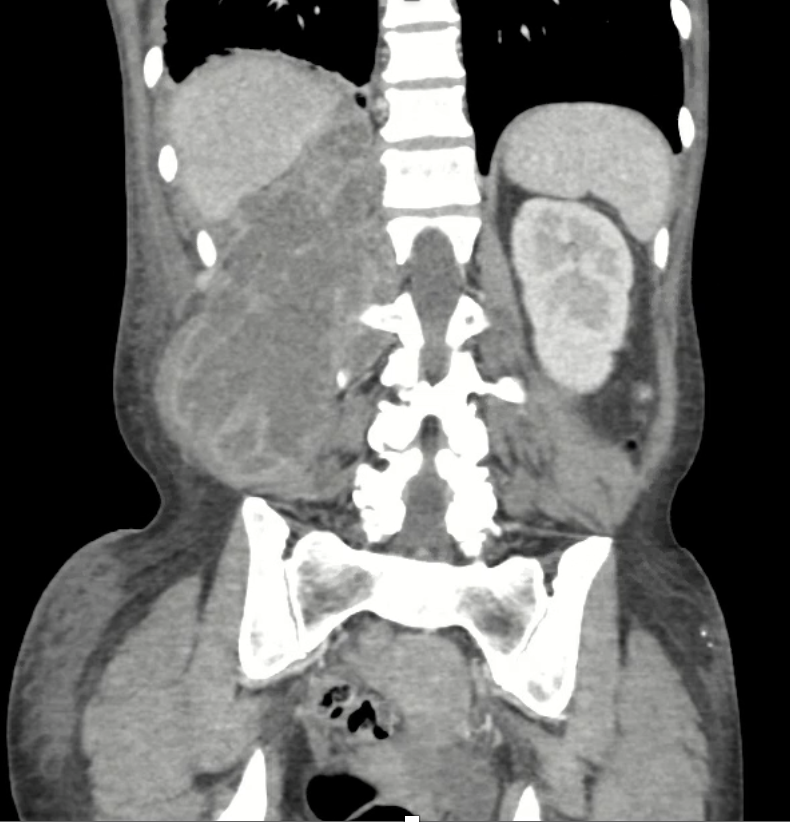
Background: Epididymitis is a common cause of scrotal pain in adults, with coliform bacteria being the most common isolated organisms in patients older than 35.
Case presentation: A 51-year-old healthy patient presented with scrotal pain and swelling, and was found to have epididymo-orchitis and bacteraemia caused by Haemophilus influenzae, which has not previously been reported as a cause of epididymo-orchitis and bacteraemia in immunocompetent patients.
Discussion: Diagnostic studies can help confirm the diagnosis and detect the causative pathogen. In all suspected cases, a urinalysis, urine culture and a urine or urethral swab for nucleic acid amplification tests (NAATs) for Neisseria gonorrhoeae and Chlamydia trachomatis should be performed. Colour Doppler ultrasonography often shows an enlarged thickened epididymis with increased Doppler wave pulsation in epididymitis. H. influenzae are pleomorphic gram-negative rods that commonly colonise the human respiratory tract and are associated with a number of clinical conditions. H. influenzae has been reported as a cause of epididymo-orchitis in prepubertal boys, and in few cases were associated with positive blood cultures. In adults, H. influenzae has been isolated before from urine samples or urethral swabs in patients with epididymitis or epididymo-orchitis.
Conclusion: This case highlights the possibility of H. influenzae causing epididymo-orchitis and bacteraemia in immunocompetent patients. Healthcare providers should consider H. influenzae in the differential diagnosis of epididymitis and epididymo-orchitis in both immunocompetent and immunocompromised patients.

|
Views: 668
HTML: 80
PDF: 536
|
Sodium-glucose cotransporter-2 (iSGLT2) inhibitors, which include dapagliflozin, canagliflozin and empagliflozin, are a class of drugs initially used in the oral treatment of diabetes, heart failure and renal failure. They target the reabsorption of glucose in the kidney. Although they bring benefit to patients with these conditions and in general produce few adverse effects, in some cases, iSGLT2 can cause serious adverse effects such as metabolic acidosis, and fungal or bacterial urinary infections. Oncology patients, who in general have a weak immune system and are usually treated with chemotherapy and/or immunotherapy, are more susceptible to this type of adverse events than other patients. For this reason, it is necessary to adequately select the patients eligible to receive this type of drug and evaluate the potential benefits for them. In this series of five cases, we present two cases of metabolic acidosis, two cases of bacterial urinary sepsis, and one case of fungal urinary sepsis that occurred in patients admitted to the Medical Oncology Department of the University Hospital of Salamanca in 2023.
|
Views: 276
HTML: 42
PDF: 194
|
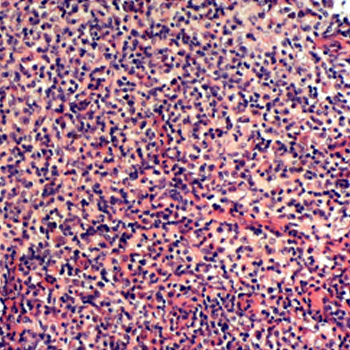
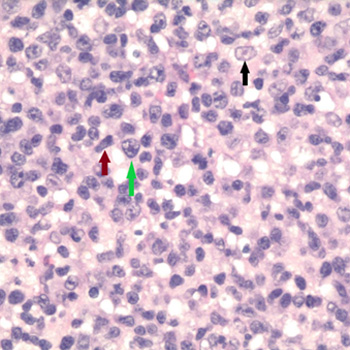
While primarily described in children, adult-onset Langerhans cell histiocytosis (LCH) has been reported, albeit infrequently. In the present scenario, we unveil a unique case of adult-onset LCH in an HIV-infected individual. After the diagnosis was made, the patient was successfully treated and demonstrated total disease remission. This case illustrates the diagnostic challenge that rare clinical entities such as LCH pose, especially in the context of an untreated HIV infection. Furthermore, the complexity of treating adult-onset Langerhans cell histiocytosis in an HIV-positive patient is highlighted, with emphasis given on a multidisciplinary approach.
|
Views: 461
HTML: 71
PDF: 339
|
Infectious mononucleosis (IM), the most common presentation of acute Epstein Barr virus (EBV) infection, typically presents with fever, pharyngitis and lymphadenopathy. We describe an unusual case of IM presenting as acute sinusitis. A 25 year-old male presented to the emergency department with worsening right frontal sinus pain along with fever, chills, and greenish nasal discharge for 3 weeks. Laboratory workup showed leukocytosis with high lymphocyte counts as well as transaminitis. Facial computerized tomography (CT) showed extensive right frontal, ethmoidal and maxillary sinusitis and antrochoanal polyp. The patient underwent endoscopy with drainage of purulent material and polyp removal. Unfortunately, cultures of the sample were not sent and bacterial infection could not be ruled out. Broad spectrum antibiotics were continued. Pathology of redundant tissue revealed large atypical lymphocytes with positive EBV-encoded RNA and lack of evidence of extranodal natural killer/T-cell (NK/T-cell) type lymphoma (ENKTCL). Tests for serum EBV IgM antibodies and EBV early Antigen antibodies were positive, indicating acute EBV infection. Lymphocytosis resolved along with significant clinical improvement at the 10-day follow up visit. Even though patient did receive antibiotics, multiple factors including isolated lymphocytosis, pathology positive for EBV with no neutrophilia were more suggestive of sinusitis caused by viral infection, EBV in this case. Lymphocytosis with fever and sore throat should prompt physicians to consider IM. There are no known reports in the literature of EBV as a causal organism for acute viral sinusitis. There are some studies relating EBV with ENKTCL. It is unknown whether this particular patient with a history of EBV sinusitis will be at high risk for nasal type lymphoma in the future. Further studies should be conducted to understand the pathogenesis and relationship between EBV and ENKTCL.
|
Views: 355
HTML: 43
PDF: 324
|
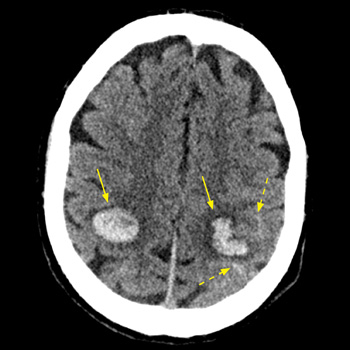
Introduction: Intracranial haemorrhage may complicate infective endocarditis, caused by ruptured mycotic aneurysms or haemorrhagic transformation of brain septic emboli. The risk of intracranial bleeding may increase with the use of non-steroidal anti-inflammatory agent (NSAIDs).
Case description: We report on a 53-year-old male patient with a past history of intravenous drug abuse, who was treated with diclofenac (75 mg IM) for a few hours of preceding fever and arthralgia. Seven hours later he was hospitalised with impaired consciousness and hemiparesis. Evaluation revealed multiple intracranial haemorrhages, at least one originating from a mycotic aneurysm. Repeated blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA), and echocardiography revealed a vegetation on the mitral valve, establishing the diagnosis of bacterial endocarditis.
Conclusion: The abrupt simultaneous multifocal intracranial bleeds shortly following the administration of NSAIDs for a few hours of febrile disease, one clearly originating from a mycotic aneurism, are exceptional. This raises a possibility of a role for diclofenac the intracranial bleeding diathesis in this unique clinical presentation. Intracranial haemorrhage in the set-up of undiagnosed infective endocarditis (IE) might be added to the long list of potential adverse outcomes of NSAID administration, and the possibility of IE should be considered before their administration for febrile disease of undetermined cause.
|
Views: 601
PDF: 739
HTML: 86
|
Varicella-zoster virus (VZV) commonly causes benign skin manifestations in children; it then establishes a latent infection and may reactivate, causing herpes zoster. The most common zoster complication is postherpetic neuralgia, but complications can also occur without a rash. VZV infection may cause neurological manifestations and even vasculopathy may occur, in both primary and reactivated VZV infection. Thrombotic complications are mainly described in children, while a few case reports have described cerebral venous sinus thrombosis (CVST), deep-vein thrombosis of the lower limbs and pulmonary embolism in adults. In this article we report the case of a young woman who developed systemic thromboembolic sequelae due to a hypercoagulable state following VZV reactivation. She had deep venous lower-limb thrombosis extended to the inferior vena cava (IVC), massive pulmonary embolism and CVST. Moreover, VZV reactivation caused an acute hepatitis and clinical manifestations suggesting viral encephalitis.
|
Views: 294
HTML: 65
PDF: 300
|
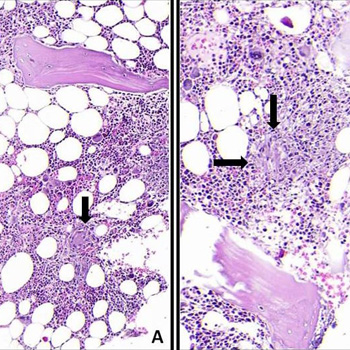
Intravesical bacillus Calmette-Guérin (BCG) is used for urothelial carcinoma. Systemic side effects are rare and commonly include organ involvement but rarely include bone marrow. We describe a patient who had received intravesical BCG and presented shortly afterwards with constitutional symptoms. Initial work-up revealed pancytopenia and immune haemolysis. He was presumptively diagnosed with systemic BCG infection and secondary warm autoimmune haemolytic anaemia. Isoniazid, rifampin and ethambutol was started. The bone marrow biopsy revealed granulomas. Within 6 weeks of treatment, the patient's clinic and laboratory results were dramatically improved. A high level of suspicion is crucial for diagnosis and treatment.
|
Views: 336
PDF: 334
HTML: 57
|
Glucocorticoid intramuscular injections are a quick, routine procedure done in an outpatient setting to relieve musculoskeletal pain quickly. However, despite being a low-risk procedure it can lead to local infections, including abscess and skin necrosis, and even more rarely, bacteraemia and multi-organ failure. In this case, we present a healthy, immunocompetent woman in her 40s diagnosed with a retroperitoneal abscess due to methicillin-resistant Staphylococcus aureus after an intramuscular injection of triamcinolone.

|
Views: 461
HTML: 53
PDF: 423
|
Long-acting (LA) cabotegravir/rilpivirine (CAB/RPV) is a complete regimen for the management of human immunodeficiency virus type 1 (HIV-1) infection to replace their oral antiretroviral therapy (ART) when they have been virologically suppressed. We present a case of successful achievement of undetectable HIV RNA viral load levels in an acquired immunodeficiency syndrome (AIDS) patient with long-standing virologic failure within two months of CAB/RPV LA initiation. This was later complicated by immune reconstitution inflammatory syndrome (IRIS) due to Mycobacterium avium-intracellulare (MAI) infection and hepatitis B virus (HBV) reactivation.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

