EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 230
HTML: 19
PDF: 160
|
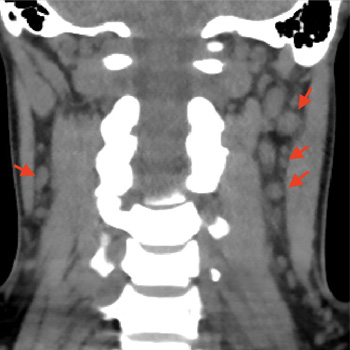
Syphilis, a disease caused by the bacteria Treponema pallidum, has a multitude of clinical manifestations and is classified into primary syphilis, secondary syphilis and tertiary syphilis, based on clinical presentations and the time elapsed since the primary infection. The secondary stage of the disease can affect multiple organs and systems, and some of these involvements may be general and non-specific, justifying its name as ‘the great imitator’. We present a case of a 30-year-old woman with a history of painful neck lymph nodes with progressive enlargement, persistent headache, weight loss, myalgia and alopecia. During investigations, stomatitis on the dorsal face of the tongue developed. A secondary study showed serum positive for rapid plasma reagin (RPR) and T. pallidum haemagglutination (TPHA), negative RPR in cerebrospinal fluid and normal MRI, thus the diagnosis of secondary syphilis was made. The patient was treated with a single dose of penicillin with complete resolution of symptoms. The case highlights the need for an exhaustive clinical examination, especially in cases presenting with non-specific and general symptoms, and raises awareness for this disease which has increased its prevalence in the last decades.
|
Views: 291
HTML: 53
PDF: 200
|
Background: Community-acquired bacterial meningitis in adults represents one of the most severe infectious diseases worldwide with potentially life-threatening medical complications. Several infectious agents can cause acute meningitis. Although group B Streptococcus is more prevalent in newborns, infection can also lead to meningitis in older adults, particularly those with underlying health issues.
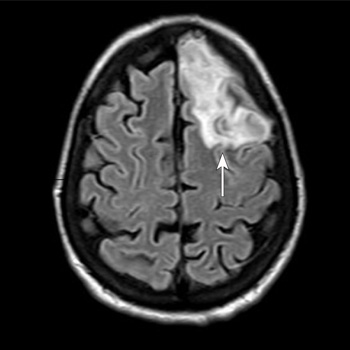
Case Description: A 53-year-old woman with a body mass index of 28.7 kg/m2, type 2 diabetes mellitus, and dyslipidaemia presented to the emergency department of Santa Maria della Stella Hospital (Orvieto, Italy) with confusion, low-grade fever, echolalia, and hyperglycaemia. Computed tomography scans of the brain revealed a hypodensity in the left anterior frontal lobe and an osteodural defect of the rhinobase. Meningitis was suspected and empiric broad-spectrum antibiotic therapy with corticosteroids and insulin were administered while the results of the cerebrospinal fluid analysis confirmed the diagnosis of group B Streptococcus meningitis. Repeat imaging at 48 hours revealed enlargement of the hypodense lesion. The frontal assessment battery indicated deficits in executive functions. Prompt treatment led to rapid clinical improvement. Following the restoration of euglycemic status and hemodynamic stabilization, a follow-up magnetic resonance imaging confirmed the ischaemic lesion and showed cerebrospinal fluid in the sella turcica. The patient was then transferred to neurorehabilitation.
Conclusions: The complex interactions among multiple risk factors resulted in an atypical clinical case of group B Streptococcus meningitis, which was promptly treated with empiric antibiotic therapy to mitigate neurocognitive deficits.
|
Views: 303
HTML: 18
PDF: 189
|
Histoplasmosis is a soil based dimorphic fungus endemic to the Midwest and Southeastern United States and is responsible for infection through inhalation of conidia. Infection is usually asymptomatic, as the fungal growth is contained by formation of granulomas. However, dissemination can occur in immunocompromised hosts due to the lack of optimal activity of interferon gamma, tumor necrosis factor-alpha (TNF-alpha) and interleukin-17. There is a significant overlap between the symptomatology of histoplasmosis and granulomatosis with polyangiitis (GPA). We are reporting a case of a 48-year-old female who presented with high grade fever, worsening generalized weakness and tachycardia. She had a previous history of bilateral cavitary lung lesions for which she was evaluated at an outside facility. As her entire infectious work up was negative and found to be positive for antineutrophil cytoplasmic antibody (ANCA), a diagnosis of GPA was made and she was initiated on rituximab infusions 7 weeks prior to her presentation to our facility. Repeat infectious work up at our facility was positive for (1,3) beta-D-glucan test and urine histoplasma antigen. Prompt discontinuation of rituximab and initiation of systemic antifungal therapy led to clinical improvement. Based on this experience we would like to highlight the association of histoplasma with ANCA positivity along with the importance of closely monitoring these patients, for possible clinical worsening after the initiation of immunosuppressive therapy, despite the negative infectious work up.
|
Views: 309
HTML: 40
PDF: 189
|
Background: Melioidosis is an infection caused by Burkholderia pseudomallei, a Gram-negative bacterium. It is a disease endemic to Southeast Asia and northern Australia although its global incidence has been rising. It most commonly infects people with certain identified risk factors such as diabetes, alcoholism, thalassemia, and underlying chronic disease involving lungs, kidney and liver. This bacterium is capable of producing a wide array of clinical manifestations ranging from asymptomatic disease to localised infections such as in the lung, bone or skin to disseminated infection.
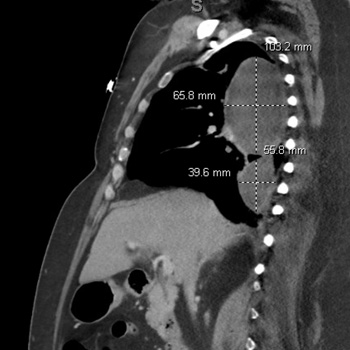
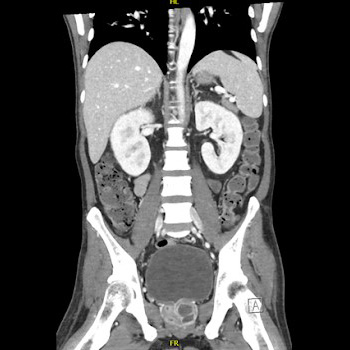
Case description: This is a case, from United Arab Emirates, of a 40-year-old male recently diagnosed with diabetes who presented with multiple abscesses and was eventually diagnosed with disseminated melioidosis. He was treated successfully with antibiotics and drainage of abscesses.
Conclusion: In non-endemic regions, melioidosis can be easily missed in common diagnostic approaches. This gap of awareness could delay the diagnosis and allow further deterioration of the patient due to complications. Thus, case reports like this can enlighten internists about changing incidences and complexity of clinical presentations, thus preparing them to better handle such patients in the future.
|
Views: 499
HTML: 35
PDF: 273
|
Background: Although there is no specific therapy for COVID-19, it is recommended that patients with severe SARS-CoV-2 infection are treated with corticosteroids and anti-IL-6 receptor monoclonal antibodies. Both COVID-19 itself and the treatment modalities mentioned above have suppressive effects on the immune system which may lead to an increased susceptibility to other infections. In patients with latent tuberculosis (TB) reactivation of TB infection after recovery from severe COVID-19 has been described. Most of these cases have occurred in parts of the world where tuberculosis is endemic.
Case description: The patient is a female in her 70s who was born and raised in Southeast Asia and has lived in the Netherlands for more than 30 years. She was treated for a severe COVID-19 requiring mechanical ventilation for several weeks and pharmaceutical treatment with corticosteroids and anti-IL-6 receptor monoclonal antibodies (Sarilumab). She recovered well. Two years later she was readmitted with symptoms of a serious pulmonary infection and meningitis. Her condition deteriorated in a short time. An active TB infection was diagnosed. Despite adequate antibiotic treatment and supportive therapy her condition worsened and four days after admission to the ICU she deceased.
Discussion: Reactivation of latent TB after recovery from a severe COVID-19 has been described several times and may occur several months after the SARS-CoV-2 infection. In this case the reactivation presented two years after COVID-19. This case illustrates that long-term follow-up of patients with latent TB that recover from a severe COVID-19 may be indicated.

|
Views: 131
HTML: 16
PDF: 144
|
Lung underdevelopment is a rare congenital anomaly with variable clinical significance and presenting symptoms. It usually manifests during childhood. We present two cases of developmental lung anomaly subtypes and discuss clinical presentation and outcomes in such patient populations.

|
Views: 404
HTML: 53
PDF: 269
|
Introduction: Kaposi’s varicelliform eruption (KVE), also known as eczema herpeticum or eczema vaccinatum, is an acute dermatosis that affects patients with chronic dermatopathies. The diagnosis is primarily clinical and is characterised by the presence of a vesicular exanthema on physical examination. The exanthema subsequently evolves into crusted lesions with typical circular ulcerations in ‘punched-out’ areas on the skin affected by the underlying dermatopathy.
Case description: We present the case of a 6-year-old patient who presented to the Paediatric Emergency department with skin lesions consistent with eczema herpeticum. The patient’s management was initially outpatient; however, due to the slow progression of the condition, hospitalisation and intravenous antiviral treatment were initiated.
Discussion: KVE affects patients with chronic dermatoses, especially atopic dermatitis. It is important to know the clinical presentation for an early suspicion. KVE is a medical emergency that requires prompt diagnosis and treatment. It can progress to secondary viraemia, which can be fatal in up to 10% of immunocompetent individuals and up to 50% of immunocompromised individuals. It is important to be aware of this condition and to start early treatment with antivirals, especially given the high prevalence of atopic dermatitis in our population. This condition is one of the most serious complications that can occur in these patients.
|
Views: 199
HTML: 21
PDF: 150
|
Kocuria kristinae is a Gram-positive commensal bacterium, rarely responsible for infection in immunocompromised patients.
A 29-year-old woman affected by intestinal pseudo-obstruction and requiring home parenteral nutrition, was hospitalised for fever and shivering during the infusion through a long-term central venous catheter (CVC).
Blood cultures were positive for K. kristinae infection. At a chest CT scan, two partially cavitated nodular lesions were evidenced. Meropenem antibiotic therapy was used locally and systemically, resulting in catheter use restoration.
A chest CT scan two months later at follow-up showed two centimetric, fibrotic and disventilatory areas replacing the previous nodular thickenings.
Kokuria kristinae was responsible for haematogenous pulmonary involvement with excavated nodules, requiring a differential diagnosis. Moreover, in the case of a CVC infection, in addition to the risk of right endocarditis, haematogenous pneumonia must also be considered.
|
Views: 245
HTML: 17
PDF: 236
|
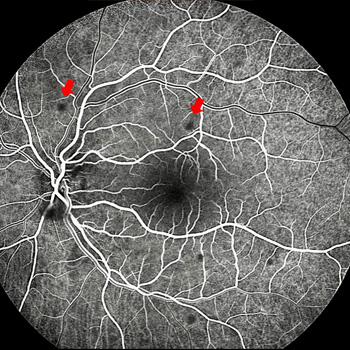
Introduction: A case of ocular bartonellosis under anti-tumour necrosis factor treatment is described.
Case description: A 29-year-old woman with psoriasis who had been on certolizumab treatment was examined with a left visual deterioration following a fever bout, malaise, and placoid erythematous rashes on her neck. As there was acute anterior uveitis in her left eye, it was recommended to stop certolizumab treatment for a possible infectious aetiology. However, her physician elected to continue the certolizumab treatment. Ten days later, the patient noticed further visual decline despite the topical steroid treatment. This time, there were scattered yellow-white small retinitis foci at the left posterior pole. Infectious agents were searched and while Bartonella henselae antibodies were negative for immunoglobulin M, the immunoglobulin G titre was 1/80. Clinical findings were improved with the systemic treatment of oral trimethoprim-sulfamethoxazole (160/800 mg twice daily for six weeks) and azithromycin (500 mg once daily for two weeks).
Discussion: Though extremely rare, ocular bartonellosis should be kept in mind in patients on anti-tumour necrosis factor treatment as rapid and accurate diagnosis may end up with an excellent visual outcome and full recovery.

|
Views: 366
HTML: 33
PDF: 256
|
Background: This report presents the influence of immunosuppression by new rheumatological therapies on hepatitis E virus infection in a 54-year-old male patient with an anti-synthetase syndrome and treatment with methotrexate and rituximab.
Case description: The patient arrived at the Emergency Department with epigastric pain, vomiting and dark urine. Initial examination revealed signs of inflammation and hepatic dysfunction. Subsequent laboratory tests and imaging confirmed acute hepatitis E infection in the context of recent initiation of rituximab therapy. Despite initial suspicion of pancreatitis, subsequent investigations ruled out pancreatic involvement. Treatment with ribavirin, along with supportive measures, led to significant clinical improvement with resolution of jaundice, ascites, and oedema.
Conclusions: This case underscores the importance of considering hepatitis E in patients with autoimmune conditions, especially when initiating immunosuppressive therapies, a situation that is not well described in scientific literature and is increasingly common, necessitating proper recognition.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

