EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 211
HTML: 21
PDF: 179
|
|
Views: 370
HTML: 28
PDF: 307
|
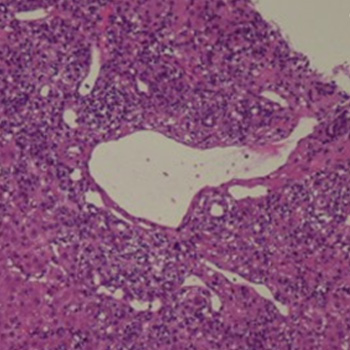
Introduction: Recently, medical interest has been growing in SARS-CoV-2 infection and its multiorgan involvement, including the liver. Up until now, a few reports have described autoimmune hepatitis (AIH) triggered by SARS-CoV-2 infection, but no data are available about the specific liver inflammatory infiltrate and cluster of differentiation. We report a case of AIH triggered by SARS-CoV-2 infection, with a particular focus on its histological and mainly immunohistochemical features.
Case description: A 60-year-old man, with a history of paucisymptomatic SARS-CoV-2 infection that occurred one month earlier, was admitted for alterations of hepatocellular necrosis and cholestasis indexes. He completed vaccination for SARS-CoV-2 a year earlier. The serologies for hepatotropic viruses were negative. The anti- smooth muscle antibodies (ASMA) and antinuclear antibodies (ANA) results were positive. Anti-liver kidney microsome (anti-LKM) antibodies and antimitochondrial (AMA) were negative. By liver biopsy, haematoxylin-eosin staining highlighted severe portal inflammation with a rich CD38+ plasma cell component, while immunohistochemical staining showed low cell CD4+ count and prevalence of CD8+ and CD3+. After biopsy, the patient started an immunosuppressant regimen, with benefit.
Discussion: We can conclude that the patient developed a type 1 AIH triggered by SARS-CoV-2 infection. The presence of CD8 T-cells at immunohistochemical examination suggests different mechanisms from classic AIH. Similar cases are described after AIH triggered by SARS-CoV-2 vaccination.
Conclusion: The AIH after SARS-CoV-2 infection developed by the patient showed a histological picture similar to a classic AIH for the abundant presence of plasma cells, and immunohistochemical features similar to those described after SARS-CoV-2-vaccination.

|
Views: 483
HTML: 37
PDF: 349
|
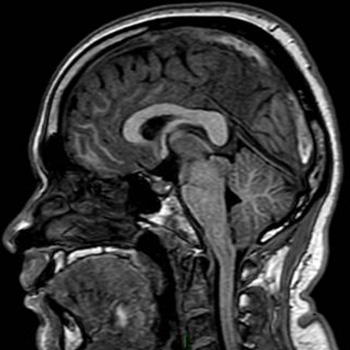
Introduction: Dysphagia in post COVID-19 patients could be caused by several factors, including reduced pharyngolaryngeal coordination due to SARS-CoV-2 tropism to the central and/or peripheral nervous system. To our knowledge, this is the first reported case of COVID-19-related dysphagia successfully treated with botulinum toxin type A injection.
Case description: We report the case of a patient with severe oropharyngeal dysphagia due to COVID-19 confirmed by fibre endoscopy. As a result, the patient required an enteral feeding tube. After two months of traditional swallowing therapies, there was only limited improvement. An electrophysiologic evaluation of the cricopharyngeal muscle was performed and showed a normal inhibition of the cricopharyngeal muscle, followed by a hypertonic rebound. Based on this result, we decided to perform a unilateral laryngeal injection of botulinum toxin type A. After the injection, the patient’s swallowing function improved significantly, allowing him to return to oral feeding.
Discussion: Newly diagnosed oropharyngeal dysphagia was found in 35.3% of hospitalised patients with COVID-19. There are several possible causes of COVID-19-associated dysphagia, including stroke, encephalitis, critical illness neuropathy, Guillain-Barré syndrome and skeletal muscle injury. In our case, since stroke was excluded by brain MRI, cranial nerve injury was a possible explanation for the difficult recovery of swallowing despite daily swallowing therapy.
Conclusion: We suggest that electrophysiology is a valid tool for the diagnosis and follow-up of patients with oropharyngeal dysphagia.
|
Views: 532
HTML: 42
PDF: 379
|
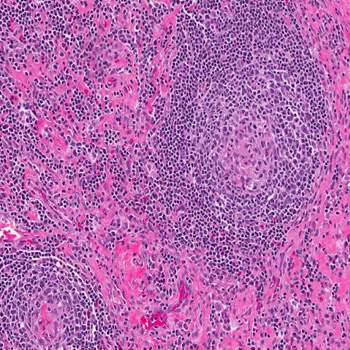
Background: Castleman disease (CD) is a rare lymphoproliferative disorder with various subtypes, including the HHV-8-negative/idiopathic multicentric CD (iMCD). The diagnosis of iMCD remains challenging due to its non-specific presentation, in the form of generalised lymphadenopathies and inflammation. Two clinical presentations have been recently defined: a severe form iMCD-TAFRO and a milder form of iMCD not otherwise specified (iMCD-NOS). identification of interleukin-6 (IL-6) as a major culprit of inflammatory symptoms led to the development of anti-IL-6 therapies, with siltuximab being the approved first-line treatment.
Case description: A 16-year-old male presented with recurrent fever, night sweats and several other non-specific symptoms. After extensive evaluations, an excisional lymph node biopsy confirmed the iMCD-NOS diagnosis. The patient received high-dose steroid therapy followed by siltuximab for four years. This treatment was well tolerated with only mild neutropenia not leading to dose adjustment. On siltuximab, the patient developed two mild COVID-19 episodes. His response to siltuximab remained effective throughout four years.
Discussion: The absence of biomarker or causal agent identification poses a diagnostic challenge requiring lymph node histopathology for a definitive diagnosis of iMCD. Anti-IL 6 (siltuximab) is the recommended frontline therapy, suppressing inflammation and halting disease progression. Intravenous administration every 3 to 6 weeks can impact patient quality of life, prompting further research for alternative treatments. High-dose steroids, rituximab, cyclosporine, tacrolimus, lenalidomide or combined chemotherapy such as rituximab-bortezomib-dexamethasone are among the considered options according to disease severity.
Conclusion: Overall, long-term siltuximab effectively controlled iMCD symptoms and was well tolerated by this young adult, who endured two mild COVID-19 episodes.
|
Views: 607
PDF: 501
HTML: 110
|
Spontaneous intracranial hypotension (SIH) is a rare cause of persistent headache, particularly among young and middle-aged people. A potentially life-threatening complication of SIH is a cerebral venous thrombosis (CVT). The authors present a case in which a patient presented with SIH complicated by CVT one week after receiving a booster dose of mRNA COVID-19 vaccine. According to our literature review, this is the first such case report.
|
Views: 608
PDF: 471
HTML: 96
|
Coronavirus 19 (COVID-19) is well known for causing acute respiratory distress syndrome. Among other systemic complications, myocarditis is a frequently reported presentation as well as complication. One systematic review reported a 14% mortality rate in patients with COVID-19 myocarditis. Endomyocardial biopsy is a definitive diagnostic test but has been a challenge to perform in most cases of COVID myocarditis due to the contagious nature of the disease. Patients presenting with new cardiomyopathy with troponin leak and arrhythmias, supported by recent COVID-19 diagnosis should be suspected for COVID-induced myocarditis. Supportive treatment has been the mainstay of treatment with limited data on immunotherapy and colchicine. Our case is about a male in his 50s who had a cardiac arrest due to ventricular fibrillations, with a positive COVID-19 test. Further workup showed severe non-ischaemic cardiomyopathy with an EF of 15–20%. He was treated with intravenous immunotherapy and colchicine. A repeat echocardiogram 3 days later showed resolution of cardiomyopathy. Our case report highlights the possible beneficial effects of immunotherapy and colchicine in viral myocarditis.

|
Views: 419
HTML: 83
PDF: 369
|
Introduction: We describe a case of remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) syndrome following administration of the ChAdOx1-S/nCoV-19 [recombinant] vaccine, suggesting a possible causal link.
Case Description: A 72-year-old man presented to his general practitioner with swollen, oedematous hands and legs 2 weeks after receiving a coronavirus vaccine. He had raised inflammatory markers but remained systemically well. He was initially presumed to have cellulitis, but his symptoms persisted despite several courses of antibiotics. Deep vein thromboses, cardiac failure, renal failure and hypoalbuminaemia were ruled out. Upon Rheumatology review, he was diagnosed as having RS3PE syndrome with the Covid vaccine suspected of being an immunogenic trigger. Following initiation of steroid therapy, his symptoms improved dramatically, as is characteristic of RS3PE syndrome.
Discussion: The pathophysiology of RS3PE is unclear. It is known to have various triggers and associations including infections, certain vaccines and malignancy. This case highlights that a coronavirus vaccine (ChAdOx1-S/nCoV-19 [recombinant] vaccine) is also a possible trigger. Factors that make the diagnosis likely include an acute onset of symptoms including pitting oedema in a typical distribution, age above 50, and unremarkable autoimmune serology. Other learning points from this case include the importance of antibiotic stewardship and the need to explore non-infectious causes of illness when antibiotics do not improve symptoms.
Conclusion: The ChAdOx1-S/nCoV-19 [recombinant] vaccine is a possible trigger of RS3PE. However, the benefits of vaccines against coronavirus outweigh the risks in the majority of patients.

|
Views: 270
HTML: 33
PDF: 264
|
|
Views: 367
HTML: 96
PDF: 324
|
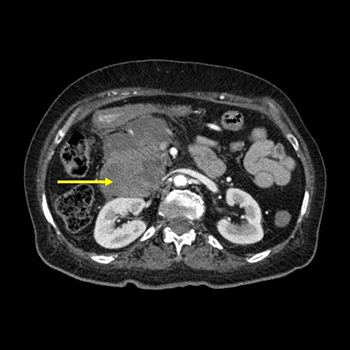
Introduction: Groove pancreatitis is a rare form of chronic pancreatitis. Its radiological diagnosis is challenging and it can be difficult to distinguish from pancreaticoduodenal malignancy.
Case description: A 64-year-old woman was admitted to our internal medicine ward after she contracted severe COVID-19 pneumonia requiring mechanical ventilation. She presented with right upper abdominal pain, and a CT scan showed pancreaticoduodenal inflammatory tissue; malignancy was ruled out.
Conclusion: Diagnosing groove pancreatitis is challenging and malignancy must be quickly excluded. No cases of COVID-19-associated groove pancreatitis have been previously described.

|
Views: 367
HTML: 69
PDF: 468
|
Rib fractures are an infrequent consequence of severe cough. In some patients, undetected rib fractures can lead to life-threatening outcomes. The case of a 73-year-old man who presented with shortness of breath and a worsening dry cough from a SARS-CoV-2 infection for 4 weeks is described. In the emergency department, he was found to be hypoxic and hypotensive. Imaging studies revealed a large right pleural effusion, multiple rib fractures, and right-sided herniation of the colon into the chest. He was admitted to the cardiothoracic intensive care unit where he underwent a flexible bronchoscopy, right video-assisted thoracoscopic surgery, evacuation of a haemothorax, complete decortication, and repair of a diaphragmatic hernia. This case is an unusual presentation of an amalgamation of rare complications resulting from an unrelenting, poorly controlled SARS-CoV-2 infection cough that prompted rapid recognition and swift action.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

