EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 754
HTML: 84
PDF: 392
|
Introduction: Pericardial effusion is common in the setting of rheumatoid arthritis (RA); however, it is rarely its first manifestation.
Case description: An 82-year-old male presented with abdominal pain, vomiting and fever. Blood analysis revealed elevated systemic inflammatory markers, and an abdominal computed tomography scan revealed non-specific alveolar condensation of the right pulmonary base and pericardial effusion subsequently quantified as medium size by transthoracic echocardiography. A large aetiological panel was requested, with the autoimmunity study revealing high levels of rheumatoid factor (RF) and anti-citrullinated cyclic peptide (anti-CCP) antibodies. Since the patient did not present articular involvement, the initial hypothesis was pericardial effusion due to pneumonia and no specific treatment for RA was started. At follow-up, the pericardial effusion recurred and a pericardiocentesis was performed. The pericardial fluid analysis was sterile, and no malignant cells were identified. A new serological study confirmed high levels of RF and anti-CCP antibodies, and immunomodulatory treatment was initiated. After one year, the pericardial effusion recurred due to non-compliance with immunomodulatory therapy. A surgical pleuro-pericardial window was performed, and the cytological study of the pericardial patch revealed submesothelial thickening and foci of perivascular lymphocytic infiltrate. The patient remained asymptomatic.
Discussion: After exclusion of a large spectrum of infectious and non-infectious causes and the relapse after suspension of immunomodulatory treatment, the most probable aetiology for the pericardial effusion remains RA.
Conclusion: Pericardial syndromes can be the first manifestation of AR even in the absence of articular symptoms and this disease must be considered in the aetiological investigation.
|
Views: 448
HTML: 65
PDF: 351
|
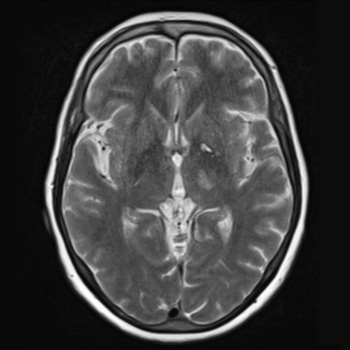
Introduction: Neurosyphilis (NS) refers to a central nervous system infection caused by Treponema pallidum. In recent years, there has been an increasing incidence of syphilis; however, NS is uncommon compared to the era before the discovery of penicillin. Manifestations are usually non-specific, ranging from asymptomatic cases to syphilitic meningitis, meningovascular syphilis, general paresis and tabes dorsalis. Meningovascular syphilis can cause an inflammatory arteritis of cerebral arteries, leading to vascular occlusion and cerebral infarction.
Case description: We report a case of an ischaemic stroke in a patient with several vascular risk factors, presenting with right hemiparesis, hemihypesthesia and dysarthria. Initial computed tomography with angiography of the head and neck was normal; however, magnetic resonance imaging of the brain revealed a thalamic and internal capsule infarct. Serum T. pallidum antibodies were positive, as well as a rapid plasma reagin test. Cerebrospinal fluid analysis confirmed the diagnosis of neurosyphilis, and the patient was treated with ceftriaxone for 14 days due to a penicillin allergy.
Discussion and conclusion: Although there is a high prevalence of stroke in patients with NS, this condition is typically underdiagnosed. Untreated NS carries a higher risk of stroke recurrence compared to other risk factors. Therefore, early diagnosis and treatment are essential. This case highlights the importance of considering NS in stroke victims, even in older patients with several additional vascular risk factors, to prevent recurrence and other complications.
|
Views: 369
HTML: 46
PDF: 248
|
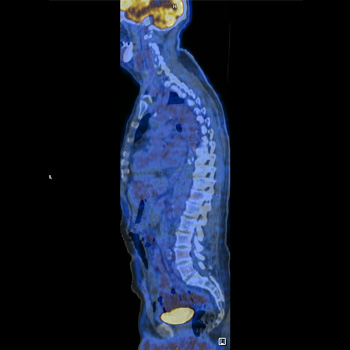
Q fever is a zoonotic infection caused by the pathogen Coxiella burnetii, and patients can present with a wide spectrum of clinical manifestations, depending on whether it is an acute or a chronic infection.
We present the case of a 61-year-old male with fatigue, posterior thoracalgia, intermittent fever, night sweats and weight loss for a month. After an extensive workup, he was diagnosed with acute Q fever with large-vessel vasculitis. The FDG-PET/CT scan suggested an active vasculitis specifically in the thoracic aorta, proximal abdominal aorta, subclavian and carotid vessels, suggesting an immunologic response to acute Q fever infection, barely reported worldwide.
|
Views: 331
PDF: 256
HTML: 31
|
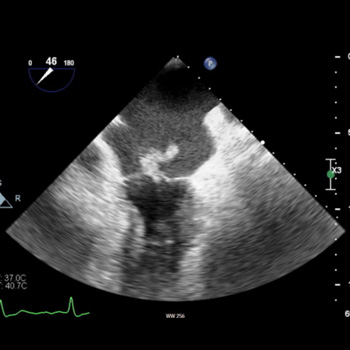
Introduction: There are very few documented cases of Escherichia coli endocarditis with cardiac abscesses in the literature. Here we describe a case presentation with diagnostic challenges and a multidisciplinary approach to management.
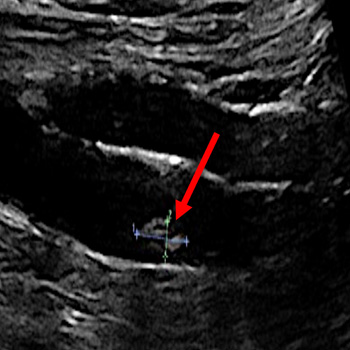
Case description: This is a rare presentation of E. coli endocarditis in a patient with a prosthetic aortic valve. Initial tests were inconclusive and further investigation with transoesophageal echocardiography was required to make the diagnosis. Despite initial improvement, the patient deteriorated and ultimately died of complications related to the presentation.
Discussion/conclusion: E. coli is a rare causative organism for endocarditis, which can itself be difficult to diagnose. A multidisciplinary approach to investigation and treatment is required when infective endocarditis is suspected. Transoesophageal echocardiography may be required to diagnose endocarditis when there is a strong clinical suspicion and risk factors present.
|
Views: 289
HTML: 40
PDF: 225
|
This report presents the clinical details and management of a 58-year-old Caucasian male with pericardial effusion and cardiac tamponade following outpatient inferior vena cava (IVC) filter removal. The patient was unresponsive and experienced cardiac arrest minutes after the procedure, requiring cardiopulmonary resuscitation. After return of spontaneous circulation he displayed somnolence, confusion and chest discomfort. Investigations revealed a large pericardial effusion, and an echocardiography confirmed cardiac tamponade. Prompt intervention involved pericardiocentesis, resulting in haemodynamic stabilisation and reduction in effusion size. The patient responded favourably with treatment. Differential diagnoses were considered and treatment options were discussed, highlighting the importance of timely recognition and appropriate intervention in managing pericardial effusion and cardiac tamponade. This report adds to the limited literature on pericardial effusion and cardiac tamponade following a scheduled outpatient IVC filter removal, emphasising the unique clinical presentation and successful management of this rare phenomenon.
|
Views: 373
HTML: 28
PDF: 292
|
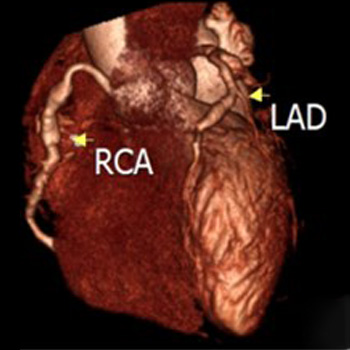
Immunoglobulin G4-related disease (IgG4-RD) is an autoimmune disease characterized by elevated serum IgG4 levels. It has the potential to affect multiple organs. Despite the diverse manifestations of IgG4-RD, the association with coronary artery disease (CAD) remains poorly understood due to limited evidence. We report the case of a 52-year-old male patient who exhibited typical angina upon exertion, accompanied by elevated serum IgG4 levels. Coronary computed tomographic angiography (CCTA) revealed the presence of pseudotumor formations surrounding and aneurysm changes affecting all coronary arteries, consistent with IgG4-RD. The patient was treated with prednisolone and azathioprine, with the possibility of additional rituximab therapy if symptomatology failed to improve. This case sheds light on the rare occurrence of IgG4-RD with coronary artery involvement and underscores the importance of recognizing this unique clinical entity for appropriate management and further research.

|
Views: 288
HTML: 52
PDF: 259
|
Background: Aortic dissection is a critical condition often presenting with acute, severe chest pain and haemodynamic instability. Early diagnosis is essential to mitigate the high mortality risk. Imaging modalities play a pivotal role in diagnosing aortic conditions, but determining the appropriate method can be challenging.
Case description: We report an asymptomatic 55-year-old female undergoing transthoracic echocardiography (TTE) for mitral and aortic valve regurgitation surveillance. Incidentally, a suspicious flow jet at the distal aortic arch was discovered, raising concerns of aortic dissection. A subsequent CT angiogram (CTA) identified this as an aortic ductus diverticulum at the aortic isthmus, not a dissection.
Discussion: Aortic dissection has a high initial 48-hour mortality, with even surgically managed cases exhibiting a 26% risk. Imaging tools such as a transoesophageal echocardiogram (TEE), CT and MRI scans are instrumental for diagnosis, with their applicability depending on the patient’s clinical situation. The aortic ductus diverticulum, a developmental outpouching, often mimics other aortic pathologies, emphasising the importance of accurate imaging interpretation.
Conclusion: Aortic ductus diverticulum presents diagnostic challenges due to its resemblance to other aortic conditions. Advancements in imaging modalities improve diagnostic accuracy, but awareness and careful interpretation are paramount to ensure timely and appropriate patient care.

|
Views: 227
HTML: 24
PDF: 182
|
This case report presents a rare case of cardiac leiomyomatosis misdiagnosed initially as submassive pulmonary embolism in a 39-year-old woman. The patient presented with syncope and hypotension, leading to an initial diagnosis of submassive pulmonary embolism. However, further investigations revealed a right-sided heart mass on echocardiogram. Surgical intervention was carried out, and the patient’s condition was successfully managed. This case emphasizes the importance of considering rare cardiac tumours in the differential diagnosis of pulmonary embolism.
|
Views: 545
HTML: 122
PDF: 226
|
Krokodil, the street name for desomorphine, has emerged as a deadly and alarming drug phenomenon in recent years. This report delves into the intricate relationship between krokodil abuse, its adverse effects on the skin and its profound impact on cardiovascular events. Our patient developed a non-healing cutaneous ulceration associated with an acute onset of cardiac arrhythmia, as well as bilateral upper extremity acute deep-vein thrombosis.
|
Views: 355
HTML: 43
PDF: 324
|
Introduction: Intracranial haemorrhage may complicate infective endocarditis, caused by ruptured mycotic aneurysms or haemorrhagic transformation of brain septic emboli. The risk of intracranial bleeding may increase with the use of non-steroidal anti-inflammatory agent (NSAIDs).
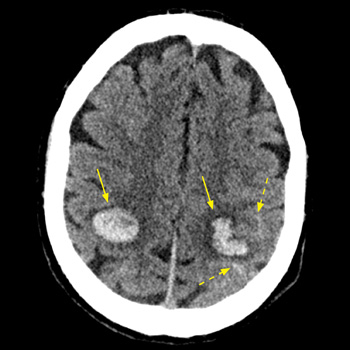
Case description: We report on a 53-year-old male patient with a past history of intravenous drug abuse, who was treated with diclofenac (75 mg IM) for a few hours of preceding fever and arthralgia. Seven hours later he was hospitalised with impaired consciousness and hemiparesis. Evaluation revealed multiple intracranial haemorrhages, at least one originating from a mycotic aneurysm. Repeated blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA), and echocardiography revealed a vegetation on the mitral valve, establishing the diagnosis of bacterial endocarditis.
Conclusion: The abrupt simultaneous multifocal intracranial bleeds shortly following the administration of NSAIDs for a few hours of febrile disease, one clearly originating from a mycotic aneurism, are exceptional. This raises a possibility of a role for diclofenac the intracranial bleeding diathesis in this unique clinical presentation. Intracranial haemorrhage in the set-up of undiagnosed infective endocarditis (IE) might be added to the long list of potential adverse outcomes of NSAID administration, and the possibility of IE should be considered before their administration for febrile disease of undetermined cause.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

