EJCRIM 2023 CiteScore
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |
Last updated on 05 May, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 231
HTML: 12
PDF: 176
|
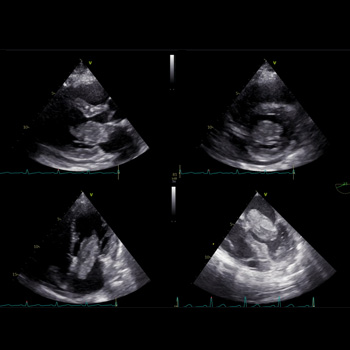
Introduction: Myxoma of the left atrium is a less typical cause of mitral obstruction. If this develops, a flash pulmonary oedema can be the first manifestation.
Case description: We present a case report of a 50-year-old woman who was admitted to our internal department because of dyspnoea. The patient overcame a stroke three years before the index hospitalisation with a negative transthoracic echocardiography. By anamnesis and physical examination, an exacerbation of COPD was assumed, and the patient was treated accordingly. As the patient showed numerous risk factors for heart failure with preserved ejection fraction, transthoracic echocardiography was performed. A large polypoid mass was found in the left atrium, which caused severe mitral obstruction. Subsequent transoesophageal echocardiography confirmed this finding. The patient underwent urgent cardiac surgery, and the tumour was successfully resected. A histological examination revealed a cardiac myxoma. After the cardiac surgery the patient felt well, and no recurrence of the tumour occurred.
Conclusions: We provide a case report of a fast-growing myxoma that was incidentally found in a patient with dyspnoea. We highlight the fast growth rate of the tumour and the potential for misdiagnosed signs of pulmonary oedema caused by mitral obstruction.
|
Views: 349
HTML: 52
PDF: 222
|
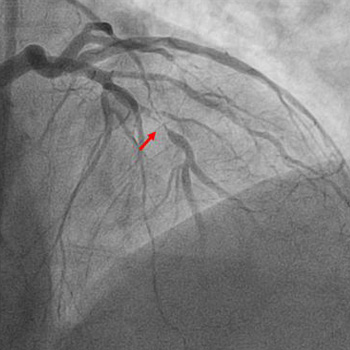
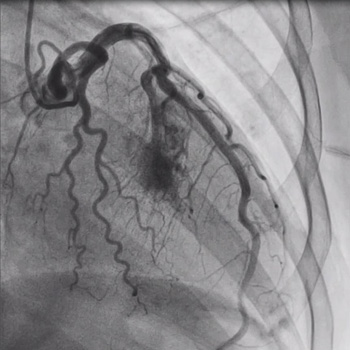
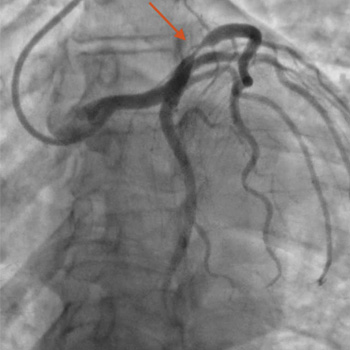
An acute ST-elevation myocardial infarction (STEMI) followed by reinfarction within a short period of time is typically due to stent thrombosis. However, a STEMI caused by occlusion of one vessel followed by a repeat infarction due to occlusion of a different vessel which was seemingly innocent a few hours earlier is extremely rare. We present the case of a 61-year-old male with a past medical history of prediabetes, hyperlipidemia, tobacco use, and gastroesophageal reflux disease who presented to the emergency department with complaints of chest pain. His initial electrocardiogram (EKG) revealed ST elevation in leads II, III and aVF with reciprocal changes in leads I and aVL. He promptly underwent cardiac catheterization and had percutaneous coronary intervention with placement of two drug-eluting stents (DES) in the right coronary artery (RCA). At that time coronary angiography revealed 50% stenosis of the left anterior descending (LAD) artery and 60% stenosis of the second diagonal branch artery. Shortly after the procedure he was asymptomatic, and the post procedure EKG demonstrated resolution of the ST elevations. However, within 2 hours he developed chest pain and was found to have new ST elevations in the anterolateral leads. Repeat cardiac catheterization revealed patent RCA stents with subtotal occlusion of the LAD and another DES was placed. After the second procedure the patient remained hemodynamically stable, EKG changes resolved, and he was kept on eptifibatide infusion for 18 hours after which he was switched to dual antiplatelet therapy and ultimately discharged home.
|
Views: 129
HTML: 10
PDF: 127
|
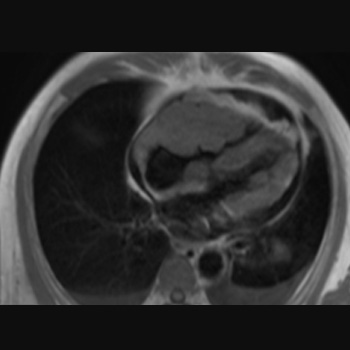
Background: This study presents a patient diagnosed with tricuspid valvular stenosis due to right ventricular lymphoma, who was treated successfully.
Case presentation: A 66-year-old man with a history of worsening shortness of breath during activity for the last three weeks sought medical attention. The patient later experienced swelling in the extremities, fluid build-up around the lungs and abdominal fluid accumulation, with no reported chest pain, fever, or weight loss. An echocardiogram found a mass in the lateral wall near the tricuspid valve of the right ventricle, leading to moderate tricuspid stenosis. The cardiac magnetic resonance imaging (MRI) revealed a lumpy, poorly defined mass that invaded the heart muscle and displayed varied enhancement after contrast administration. Suspicion arose for a malignant tumour or metastatic lesion due to its features and contrast uptake capability. A percutaneous biopsy was carried out on the mass in the right ventricle to confirm the diagnosis. The pathology report indicated a diagnosis of non-Hodgkin’s lymphoma. After being diagnosed, the patient underwent chemotherapy using the R-CHOP regimen. Over time the symptoms improved, and echocardiograms revealed a decrease in the size of the tumour. After undergoing six rounds of chemotherapy, a cardiac MRI four months later showed no signs of a tumour. After that, the patient resumed their regular activities.
Conclusion: Right ventricular tumours are mostly malignant lesions and often have an inferior prognosis. Early diagnosis with imaging techniques and myocardial biopsy is necessary to deliver life-saving treatment quickly.
|
Views: 421
HTML: 37
PDF: 274
|
Introduction: Combination-based adjuvant chemotherapy utilising capecitabine and oxaliplatin is widely used in gastric cancer treatment. Rare but severe cardiac events such as prolonged QT, cardiac arrest and cardiogenic shock can result from their use.
Case description: A 45-year-old female with gastric adenocarcinoma was started on capecitabine-oxaliplatin chemotherapy one week before presenting to the emergency department with weakness. Blood pressure was 78/56 mmHg, heart rate 140 bpm and oxygen saturation 85%. She became unresponsive with pulseless ventricular fibrillation; CPR was initiated with immediate intubation. She received two shocks with a return of spontaneous circulation. Laboratory tests revealed serum potassium (3.1 mmol/l), magnesium (1.1 mg/dl) and troponin (0.46 ng/ml). An EKG revealed sinus tachycardia with a prolonged QT interval (556 ms). The combined effects of capecitabine, oxaliplatin and electrolyte abnormalities likely contributed to the QT prolongation. An echocardiogram demonstrated an ejection fraction of 10%–15%. An emergent right-heart catheterisation showed right atrial pressure of 10 mmHg and pulmonary artery pressure of 30/18 mmHg; cardiac output and index were not recorded. An intra-aortic balloon pump was placed, and she was admitted to the ICU for cardiogenic shock requiring norepinephrine, vasopressin and dobutamine. A repeat echocardiogram showed a significantly improved ejection fraction of 65%, and she was discharged.
Discussion: Capecitabine and oxaliplatin cardiotoxicity is an exceedingly rare occurrence, with both drugs reported to cause QT prolongation.
Conclusion: Healthcare providers must recognise the QT prolongation effects of capecitabine and oxaliplatin, leading to life-threatening cardiac arrhythmias.
|
Views: 350
HTML: 18
PDF: 241
|
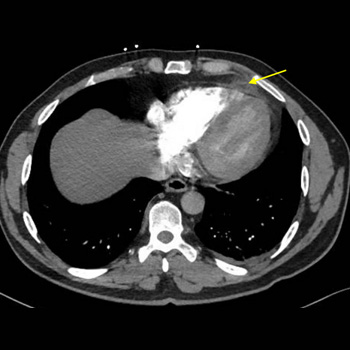
Background: Epipericardial fat necrosis (EFN) is a rare and self-limiting cause of acute chest pain. We describe a case of EFN in a patient with a recent coronavirus disease (COVID-19).
Case Presentation: A 55-year-old male presented with a sudden onset of left-sided pleuritic chest pain for the past two days. The patient was diaphoretic, tachypneic, and tachycardic. Acute coronary syndrome was ruled out. A computed tomography (CT) pulmonary angiogram revealed an ovoid encapsulated fatty mass surrounded by dense appearing tissue. Patient symptoms improved remarkably with a short course of non-steroidal anti-inflammatory drugs (NSAIDs).
Discussion: EFN typically presents with a sudden onset of excruciating chest pain. Misdiagnosis, under-diagnosis, and mismanagement are unavoidable. EFN is incidentally diagnosed on CT scan. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infects visceral adipose tissue and appears to increase the risk of EFN by promoting inflammatory cytokine production and death of adipocytes.
Conclusion: EFN is a rare cause of acute chest pain. SARS-CoV-2 is likely to induce EFN. This rare clinical entity should be considered in the differential of acute chest pain especially in patients with active or recent COVID-19.
|
Views: 256
HTML: 12
PDF: 243
|
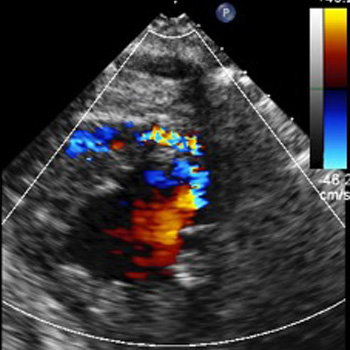
A 56-year-old African American female was under evaluation for coronary artery disease by a cardiologist due to her complaints of intermittent chest pain. She underwent an outpatient echocardiogram and was found to have an ejection fraction of 20–25% with global left ventricular hypokinesis. Due to this finding along with her ongoing chest pain, she was referred to the emergency department for further evaluation. Her electrocardiogram showed changes suggestive of ischaemia and her cardiac troponins were mildly elevated, so she underwent an urgent cardiac catheterisation. The angiography confirmed the reduced ejection fraction and global left ventricular hypokinesis, but also demonstrated a large coronary cameral fistula (CCF) extending from the first septal branch into the left ventricle. She was then diagnosed with non-ischaemic cardiomyopathy and heart failure with reduced ejection fraction secondary to the CCF. In this report, we illustrate a frequently encountered clinical scenario in which a patient presented with chest pain and EKG findings indicative of ischaemic cardiomyopathy. The patient also had several risk factors for coronary artery disease, however further investigation revealed an alternative diagnosis.
|
Views: 332
HTML: 23
PDF: 184
|
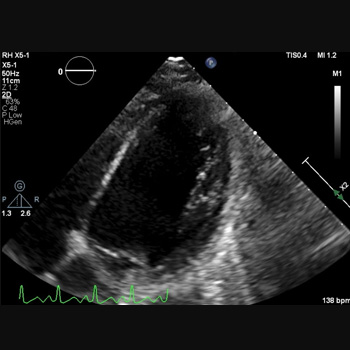
Acute myocardial infarction can result in various mechanical complications, although they have become rare with the advent of reperfusion therapies. Among these complications, ventricular septal rupture (VSR) and left ventricular aneurysm (LVA) are infrequent but life-threatening conditions associated with high morbidity and mortality. We present a rare case of a 67-year-old male with acute myocardial infarction who developed concomitant apical LVA and ventricular septal rupture.
|
Views: 390
HTML: 17
PDF: 258
|
Anagrelide is a medication primarily used to manage thrombocytosis, an abnormal increase in platelet levels in the blood. It is often prescribed for patients with myeloproliferative disorders, such as essential thrombocythaemia (ET). Given the heightened susceptibility to thromboembolism associated with this condition, the primary emphasis in treatment revolves around reducing the risk of thrombotic events through the administration of cytotoxic agents. While anagrelide is generally effective in reducing platelet counts, it comes with potential side effects, including an increased risk of certain thrombotic events. Anagrelide acts by inhibiting megakaryocyte maturation and platelet release, thereby reducing platelet production. However, this platelet-lowering effect may be accompanied by an increase in platelet activation and reactivity, which could contribute to a prothrombotic state. We present a case of a 60-year-old female with a history of ET, managed with anagrelide and hydroxyurea therapy, who experienced an acute ST-elevation myocardial infarction.

|
Views: 198
HTML: 9
PDF: 197
|
Spontaneous bleeding into the upper airways is a rare and potentially life-threatening complication of chronic anticoagulation. There are scarce cases in the literature demonstrating upper airway haematomas secondary to warfarin use, which is the predominant anticoagulant used by clinicians despite having a complex pharmacokinetic and pharmacodynamic profile. We report a compelling case featuring warfarin-induced sublingual haematoma, managed conservatively through the reversal of anticoagulation using fresh frozen plasma complemented by vigilant monitoring within the Intensive Care Unit (ICU).

|
Views: 377
HTML: 16
PDF: 301
|
Introduction: Pulmonary artery aneurysm (PAA) is a rare abnormality of pulmonary vasculature. It can be idiopathic or secondary to various pathologies, frequently with multiple factors leading to its formation. We report the case of a man with concomitant sarcoidosis and PAA.
Case description: A 75-year-old male with a diagnosis of pulmonary sarcoidosis was referred to the Cardiology department due to heart failure with reduced left ventricular ejection fraction (LVEF). The transthoracic echocardiogram revealed mildly reduced LVEF, aortic root and pulmonary artery (PA) dilatation, and no signs of pulmonary hypertension (PH). Cardiac magnetic resonance imaging was performed, revealing mild left ventricular dilation, LVEF of 40%, main PA dilation (43 mm) and a pattern of late gadolinium enhancement suggestive of cardiac sarcoidosis. At follow-up, a thoracic computed tomography (CT) angiography scan revealed ascending aorta ectasia and giant main PA aneurysm (60 mm). A right heart catheterisation was performed, and a mean PA pressure of 34 mmHg was obtained. Given the clinical context, the patient was considered to have PH due to lung disease and left heart disease, and PAA was possible due to vascular granulomatous involvement by sarcoidosis.
Conclusion: PAA is a rare finding and mostly occurs in the setting of PH. Sarcoidosis is a granulomatous disease that mostly affects the lungs, but the sarcoid involvement of great vessels has been described. In this clinical case, the probable cause for the PA fragility leading to aneurysm formation remains sarcoid vascular infiltration, regarding the discrepancy between the PA dimensions and mildly elevated PA pressure.
| 2.1 = | 1.762 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2024, Published by SMC Media srl, Italy - Privacy policy

