Keywords
Paraganglioma, phaeochromocytoma, bladder resection, SDHB
Abstract
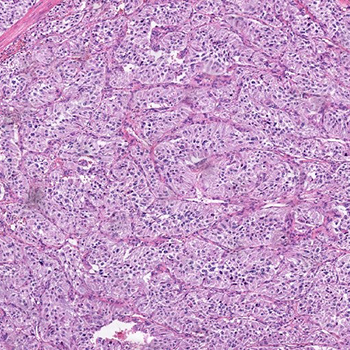
A 22-year-old female presented with a twelve-year history of intensifying paroxysms of anxiety, palpitations and recurrent syncope following micturition. The patient was referred to endocrinology upon discovery of hypertension. Extended family history revealed metastatic phaeochromocytoma and paraganglioma in two grand-uncles. Clinical examination revealed hypertension, mean 24hr ambulatory blood pressure of 150/100mmHg. Supine plasma normetanephrines were markedly elevated with a raised 3-methoxytyramine, plasma metanephrines were normal. Computed tomography identified a 4.4cm mass at the right inferolateral margin of the bladder wall. Scintigraphic imaging confirmed unifocal bladder lesion uptake with no additional metastatic lesions. Following pre-operative alpha blockade, the patient underwent a partial cystectomy. Histology confirmed a paraganglioma, SDHB staining was lost in neoplastic cells consistent with an SDHB-related paraganglioma. Plasma normetanephrine, 3-methoxytyramine and blood pressure returned to normal postoperatively. Genetic screening identified a germ line heterozygous SDHB gene variant c.723C>G. Bladder paragangliomas are a rare but important differential to consider when investigating post-micturition syncope. Extended family history should be sought and suspicion for a genetic cause should be raised, especially when presenting at a young age. This is the first reported case describing phaeochromocytoma or paraganglioma with the SDHB gene variant c.723C>G.
References
Views: 686
HTML downloads: 143
PDF downloads: 482
Published:
2022-09-28
Issue:
2022: Vol 9 No 9
(view)






