Keywords
Non-Hodgkin lymphoma, CNS lymphoma, pituitary macroadenoma, sellar mass
Abstract
Non-Hodgkin lymphomas of the hypothalamus and pituitary are rare. They usually remain clinically silent until onset of compressive features affecting surrounding structures. When symptomatic, patients most commonly present with diabetes insipidus, headaches, ophthalmoplegia and/or bilateral hemianopia.
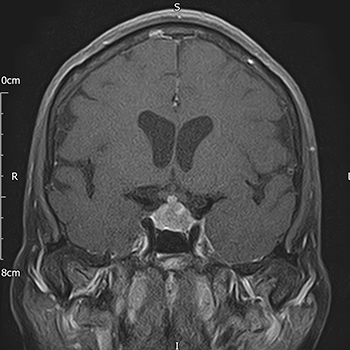
We report a case of a 67-year-old Caucasian female with a history of B-cell lymphoma in complete remission. She presented with left oculomotor nerve palsy and was subsequently found to have a sellar/suprasellar mass lesion on MRI. Alongside hypocortisolism and hypogonadotropic hypogonadism, she developed transient diabetes insipidus during her illness. Her clinical course was characterized by rapid intracranial progression of the sellar mass. MR spectroscopy suggested a diagnosis of lymphoma. Diagnostic biopsy confirmed high-grade diffuse large B-cell CNS lymphoma; this changed the definitive management from surgical excision to chemotherapy. Despite treatment, she succumbed to her illness within 7 months of initial presentation.
This case highlights the aggressive nature of CNS lymphomas and the need for a high index of suspicion in an unusual presentation of sellar/suprasellar mass lesions.
References
Views: 614
HTML downloads: 136
PDF downloads: 367
Published:
2021-12-23
Issue:
2021: Vol 8 No 12
(view)






