Keywords
Aromatase inhibitors, breast cancer, cutaneous adverse events, Sweet’s syndrome
Abstract
Background: Breast cancer is the most commonly diagnosed cancer in women, mainly at an early stage, allowing treatment with curative intent. Aromatase inhibitors are widely used in the adjuvant treatment of oestrogen receptor-positive breast cancer, mainly in postmenopausal women. The most frequent adverse events associated with these therapies are musculoskeletal symptoms and an increased risk of bone fractures. Cutaneous adverse events have been rarely described. Sweet’s syndrome can present as an idiopathic disorder in addition to being malignancy-associated or drug-induced.
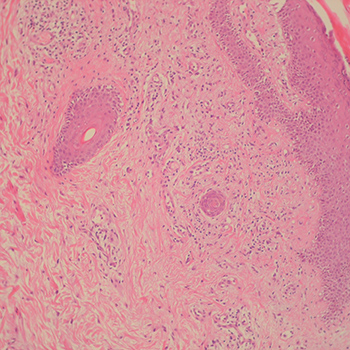
Case presentation: We report the case of a 69-year old woman, diagnosed with early stage breast cancer, who underwent breast-conserving surgery, followed by adjuvant radio and endocrine treatment with letrozole 2.5 mg daily, for a foreseeable duration of 5 years. Three months after starting letrozole, she presented with sudden fever and exuberant and painful erythematous skin papules and plaques on her upper body. After a full work-up and exclusion of other potential causes, a skin biopsy confirmed the presence of dermal oedema and a diffuse neutrophilic infiltrate, suggesting Sweet’s syndrome. After discontinuation of letrozole and treatment with corticosteroids, the patient fully recovered. She resumed adjuvant treatment with tamoxifen, without symptom recurrence.
Conclusions: Sweet’s syndrome is a rare condition and an association with aromatase inhibitors has not been previously reported. Although its occurrence has already been observed in the onset of malignancies such as breast cancer, aromatase inhibitors must be added to the list of potential causes of drug-induced Sweet’s syndrome.
References
Views: 1130
HTML downloads: 109
PDF downloads: 451
Published:
2020-02-07
Issue:
2020: Vol 7 No 3
(view)






