EJCRIM 2023 CiteScore
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by


|
Views: 15058
HTML: 260
PDF: 1560
|
Younger patients with COVID-19 may experience an exaggerated immune response to SARS-CoV-2 infection and develop cytokine release syndrome (CRS), which may be life threatening. There is no proven antiviral therapy for COVID-19 so far, but profound immunosuppression has recently been suggested as a treatment for COVID-19-associated CRS. We present a case of life-threatening CRS caused by COVID-19 infection with a favourable response to immunosuppressive therapy with tocilizumab (TCZ). The rapid clinical and biochemical improvement following TCZ administration suggests that treatment with immunotherapy can be life-saving in selected patients with COVID-19-induced CRS.
|
Views: 1707
HTML: 130
PDF: 832
|
Cytokine release syndrome (CRS) is a systemic inflammatory response that can be triggered by many factors such as infections. CRS in patients with coronavirus disease 2019 (COVID-19) is life-threatening and can occur very rapidly after COVID-19 diagnosis. Tocilizumab (TCZ), an interleukin?6 (IL-6) inhibitor, may ameliorate the CRS associated with severe COVID?19 and thus improve clinical outcomes. We present a case of life-threatening CRS caused by COVID-19 infection successfully treated with TCZ.
|
Views: 8281
HTML: 410
PDF: 1574
|
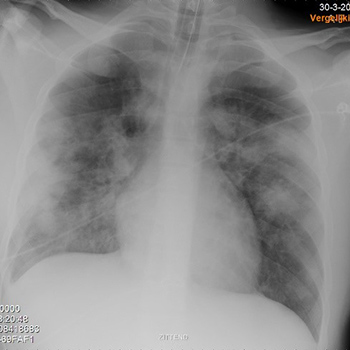
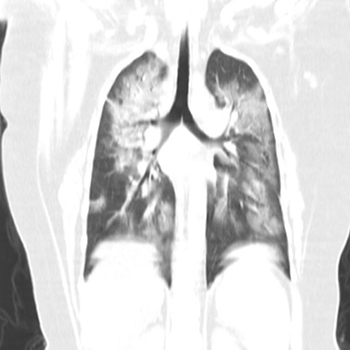
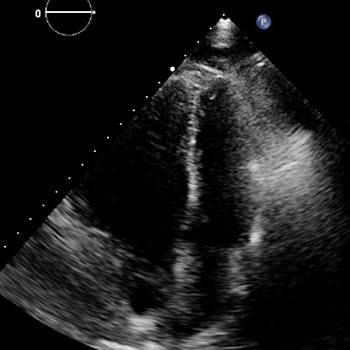
COVID-19 is a novel viral disease caused by SARS-CoV-2. The mid- and long-term outcomes have not yet been determined. COVID-19 infection is increasingly being associated with systemic and multi-organ involvement, encompassing cytokine release syndrome and thromboembolic, vascular and cardiac events. The patient described experienced unusually rapid development of pulmonary hypertension (PH) and right ventricular failure after recent severe COVID-19 pneumonia with cytokine release syndrome, which initially was successfully treated with methylprednisolone and tocilizumab. The development of pulmonary hypertension and right ventricular failure – in the absence of emboli on multiple CT angiograms – was most likely caused by progressive pulmonary parenchymal abnormalities combined with microvascular damage of the pulmonary arteries (group III and IV pulmonary hypertension, respectively). To the best of our knowledge, these complications have not previously been described and therefore awareness of PH as a complication of COVID-19 is warranted.
|
Views: 1602
HTML: 158
PDF: 858
|
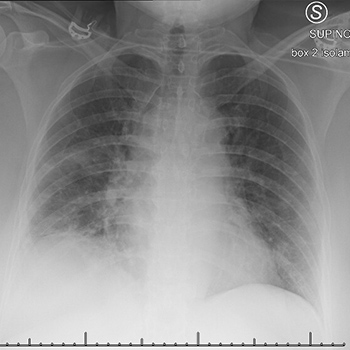
On 11 March 2020, the WHO declared COVID-19 a pandemic and global health emergency. We describe the clinical features and role of ultra-low-dose chest computed tomography (CT) and bronchoscopy in the diagnosis of coronavirus disease (COVID-19). In our patient, who was highly suggestive clinically and radiologically for COVID-19, we had two false-negative results for nasopharyngeal and oral swab reverse-transcriptase polymerase chain reaction (RT-PCR) assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Eventually, we confirmed the diagnosis using bronchoscopy and bronchoalveolar lavage (BAL).
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2023, Published by SMC Media srl, Italy - Privacy policy

