EJCRIM 2023 CiteScore
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 433
HTML: 44
PDF: 213
|
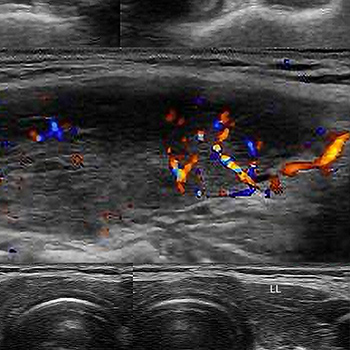
A 32-year-old woman presented to the outpatient clinic with persistent fever, anterior neck pain, and palpitations over the past week which developed 2 days after she had received the first dose of the Pfizer/BioNTech SARS-CoV-2 mRNA vaccine. On examination, the patient’s heart rate was 140 beats per minute and the thyroid gland was tender on palpation. Laboratory studies showed a low serum TSH level with elevated free thyroxine. Thyroid ultrasound revealed low-echoic lesions compatible with the site of tenderness. The patient was diagnosed with subacute thyroiditis and treatment was initiated with acetaminophen and propranolol, which resulted in symptom resolution within 2 weeks. Clinicians should be aware that subacute thyroiditis may occur within a few days following COVID-19 vaccination, especially in patients with anterior cervical pain with no significant abnormal pharyngeal findings and/or severe palpitations, because differentiating them from early non-specific adverse reactions can be challenging.

|
Views: 491
HTML: 55
PDF: 296
|
ntroduction: Non-episodic angioedema associated with eosinophilia (NEAE) has been reported primarily in young East Asian women and is characterized by a single episode of persistent limb oedema, peripheral eosinophilia, and transient joint pain. Although there are reports of eosinophilia disease after coronavirus disease 2019 (COVID-19), the occurrence of NEAE has not been previously reported.
Case description: A 29-year-old Japanese woman, with a history of allergic rhinitis and atopic dermatitis, sought a medical consultation for persisting oedema of the extremities, which developed about 2 weeks after she contracted COVID-19. Physical examination revealed symmetrical non-pitting oedema with peripheral predominance. Laboratory examination revealed a blood eosinophil count of 7536/µl. The patient was diagnosed with NEAE and a 7-day course of prednisolone (15 mg/day) was initiated, with rapid improvement in the oedema and no recurrence on follow-up.
Discussion: The exact aetiology of NEAE is unknown, but it may develop after infection or drug exposure. Eosinophilic disease after COVID-19 infection has been reported and, therefore, eosinophilic angioedema should be considered in the differential diagnosis of non-pitting oedema of the extremities after a COVID-19 infection. Early diagnosis of NEAE is important as rapid improvement can be achieved with low-dose steroid treatment.
Conclusion: NEAE can develop after COVID-19 and should be considered in the differential diagnosis of non-pitting oedema of the extremities.
|
Views: 583
HTML: 112
PDF: 326
|
Treatment strategies for patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) continue to be heavily researched and ever-changing. Recent data has suggested that combination therapy with dexamethasone, remdesivir and baricitinib could decrease the severity and length of illness in patients with severe SARS-CoV-2. However; the data regarding the safety and side effects related to this combination therapy are limited to case reports. The purpose of this case report is to highlight a potentially life-threatening side effect of one or all medications mentioned above.
|
Views: 883
HTML: 424
PDF: 594
|
Tacrolimus is commonly used as a prophylactic against acute rejection in transplant patients. Tacrolimus toxicity has numerous presentations that have been well documented in the literature and can be induced by a wide variety of agents. We present a novel case of tacrolimus toxicity in a cardiac transplant patient induced by outpatient treatment for COVID-19 pneumonia with ritonavir-nirmatrelvir, which was successfully treated with phenytoin therapy.

|
Views: 729
HTML: 225
PDF: 291
|
Introduction: mRNA COVID-19 vaccines are very safe, but rare adverse events such as transverse myelitis have been reported after COVID-19 vaccination.
Case Description: We report the case of 50-year-old man who presented with progressive lower extremity weakness, back pain and urinary retention after his second dose of the Pfizer COVID-19 vaccine. MRI of the spine revealed longitudinally extensive transverse myelitis (LETM). He recovered completely after treatment with intravenous methylprednisone and physical therapy.
Discussion: This case highlights the rare association between LETM and COVID-19 vaccines and encourages clinicians to maintain a high index of suspicion for prompt diagnosis and treatment.
|
Views: 689
HTML: 86
PDF: 328
|
Introduction: Hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome is a leading cause of maternal mortality. The emergence of Coronavirus disease 2019 (COVID-19) has led to challenges in diagnosing HELLP syndrome due to overlapping clinical and laboratory presentations. We report a case of HELLP syndrome complicated by COVID-19 infection.
Case Description: An otherwise healthy pregnant 31-year-old female presented with fever, myalgia, and headache. She was found to be COVID-positive with laboratory signs of HELLP syndrome. Symptoms and laboratory findings trended toward normal post-partum confirming the diagnosis of HELLP syndrome.
Discussion: A prompt diagnosis of HELLP syndrome is essential to avoid maternal and fetal complications. Clinicians should be aware of the similarities in presentation between HELLP syndrome and COVID-19 for timely diagnosis and treatment.

|
Views: 555
HTML: 189
PDF: 268
|
We describe four cases of COVID-19 infection during the Omicron wave, in patients treated with anti-CD20 monoclonal antibodies. All cases follow a similar biphasic clinical course consisting of respiratory deterioration, which occurred a few weeks after convalescence from initial mild to asymptomatic infection. Possible explanations are discussed.

|
Views: 580
HTML: 92
PDF: 468
|
Introduction: Several immune-mediated side effects have been reported with COVID-19 vaccines, including myocarditis.
Case description: A 27-year-old woman with a past medical history of mild COVID-19, developed adult-onset Still’s disease (AOSD) with salmon-pink flagellate erythema, polyarthritis, a sore throat, myocarditis and haemophagocytic lymphohistiocytosis after receiving two doses of the BNT162b2 vaccine (Pfizer®, BioNTech®). Despite the initial efficacy of high-dose pulses of methylprednisolone, inflammatory markers rose as soon as de-escalation of corticosteroids was attempted, warranting initiation of biologics targeting the interleukin (IL)-1/6 axis, which allowed sustained remission of the disease despite withdrawal of corticosteroids.
Discussion: To our knowledge, this is the first case of AOSD with both haemophagocytic lymphohistiocytosis and cardiac magnetic resonance imaging-proven myocarditis triggered by COVID-19 vaccination, successfully treated with steroids and biologics targeting the IL-1/IL-6 axis. The pathophysiological process by which COVID-19 vaccination can lead to AOSD is still unknown, although it has been reported that the spike protein may act as a pathogen-associated molecular pattern and thus induce an overproduction of pro-inflammatory cytokines of the innate immune system (e.g., IL-1, IL-6 or IL-18).
Conclusion: Targeting the IL-1/6 axis is effective for the treatment of severe steroid-refractory BNT162b2 vaccine-induced adult-onset Still’s disease. At a population level, the favourable benefit/risk ratio of COVID-19 vaccination remains indisputable.
|
Views: 619
HTML: 68
PDF: 286
|
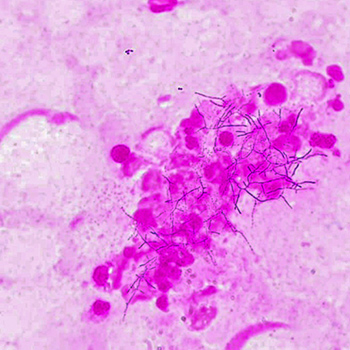
Secondary bacterial pneumonia infection is frequent in COVID-19 patients. Nocardia are responsible for opportunistic pulmonary infections especially after steroid treatment. We describe a case of pulmonary nocardiosis following critical COVID-19 pneumonia in an 83-year-old male. Two weeks after initiation of dexamethasone 6 mg/L, the patient developed a new episode of acute dyspnea. The sputum cultures identified Nocardia cyriacigeorgica. In spite of intravenous imipenem and cotrimoxazole treatment the patient died. Physicians should be aware of the possibility of nocardiosis in case of deterioration of respiratory status of severe COVID-19 inpatients and perform Nocardia evaluation. This evaluation requires prolonged culture.

|
Views: 431
HTML: 45
PDF: 239
|
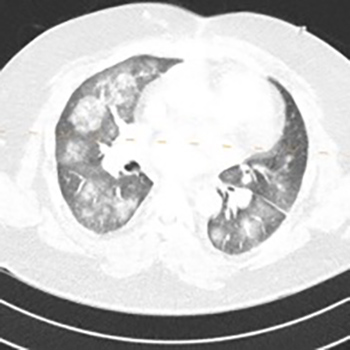
Platypnoea-orthodeoxia syndrome (POS) is a condition characterized by dyspnoea and hypoxaemia while sitting or standing, which improves during decubitus. It is usually caused by intracardiac right-to-left shunting through a patent foramen ovale but may also occur due to pulmonary ventilation-perfusion mismatch of other aetiologies. A new cause of POS was recently described: SARS-CoV-2 pneumonia. We report the case of a 62-year-old man admitted for SARS-CoV-2 pneumonia with respiratory failure. Chest computed tomography angiography showed pulmonary thromboembolism and parenchymal lung changes compatible with COVID-19. He had worsening dyspnoea in a sitting position, relieved by assuming the dorsal position. He was diagnosed with POS after other causes were excluded. POS is an underdiagnosed complication of COVID-19 and is manageable with respiratory rehabilitation.
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2023, Published by SMC Media srl, Italy - Privacy policy

