ABSTRACT
Medullary thyroid carcinoma (MTC) is a rare and challenging type of thyroid cancer originating from parafollicular cells (C cells) that produce calcitonin. Diagnosing and monitoring this carcinoma can be complex due to its unique biomarkers. Procalcitonin (PCT), a precursor of calcitonin, and carcinoembryonic antigen (CEA) are important markers for MTC. Elevated PCT levels, particularly when they remain high post-infection treatment, and elevated CEA levels are significant indicators for suspecting MTC. This report emphasises the diagnostic and prognostic importance of these biomarkers in MTC, highlighting their roles in detecting and monitoring disease progression. Integrating PCT and CEA measurements into routine clinical practice can enhance detection, provide understanding of therapeutic responses and aid in the effective management of MTC.
KEYWORDS
Procalcitonin, calcitonin, medullary thyroid carcinoma, sigmoid colon tumour, carcinoembryonic antigen (CEA)
LEARNING POINTS
- Procalcitonin (PCT) is a more stable and reliable biomarker than calcitonin for diagnosing and monitoring medullary thyroid carcinoma (MTC).
- Elevated carcinoembryonic antigen (CEA) levels effectively monitor MTC progression, especially when calcitonin levels are inconsistent.
- Incorporating PCT and CEA measurements into routine practice enhances MTC management, providing reliable biomarkers for diagnosis and monitoring.
INTRODUCTION
Medullary thyroid carcinoma (MTC) is a rare form of thyroid cancer originating from parafollicular cells (C cells) that produce calcitonin. This carcinoma poses significant diagnostic and therapeutic challenges due to its unique biomarkers[1]. Procalcitonin (PCT), a precursor of calcitonin, has become a crucial marker not only for bacterial infections but also for MTC, especially when its levels persistently elevate post-infection treatment. Similarly, carcinoembryonic antigen (CEA), a glycoprotein involved in cell adhesion, serves as another essential tumour marker for monitoring MTC[2]. This report explores the diagnostic and prognostic importance of PCT and CEA in the context of MTC.
CASE DESCRIPTION
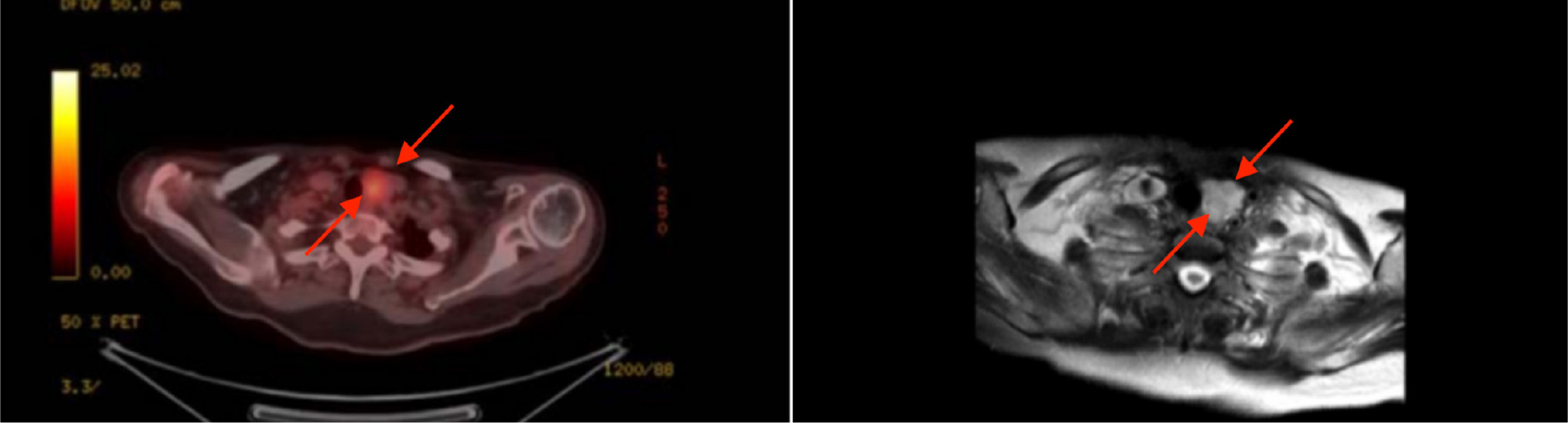
An 80-year-old female presented to the emergency department with high fever, generalised body weakness, hypotension and high procalcitonin levels (16.7 ng/ml). The patient was administered prophylactic broad-spectrum antibiotics, supplemental oxygen and fluids. Blood and urine cultures were confirmed to be sterile, yet high procalcitonin levels persisted. The patient had a previous history of papillary thyroid carcinoma 25 years previously and was treated with radical thyroidectomy, thus the significance of the concurrent testing of calcitonin to rule out thyroid pathologies was overlooked. Additionally, the patient was diagnosed with pleural and pericardial effusion and was treated accordingly with diuretics. Blood tests showed haematocrit test 25%, haemoglobin 7.5 g/dl, aspartate transferase 240 U/l, alanine transaminase 210 U/l, gamma-glutamyl transferase 310 U/l, international normalised ratio 1.96, albumin 1.9, pro b-type natriuretic peptide 9,880 pg/ml and ionised calcium 2.90 mg/dl. Positron emission tomography/computerised tomography (PET-CT) (Fig. 1) clarified that the patient had a left thyroid nodule, implying that the prior history of radical thyroidectomy was misleading and inaccurate. Further testing concluded that the patient had MTC secondary to the growth of tissue remnants post-thyroidectomy. Additionally, the PET-CT (Fig. 2) scan revealed a tumour in the sigmoid colon, which was confirmed as early-stage sigmoid cancer through a biopsy. The patient also presented with elevated levels of CEA at 69.29 ng/ml and CA19-9 at 29.34 ng/ml.

(click to enlarge)
Figure 1. PET CT showing a nodule on the left thyroid gland tissue.
(click to enlarge)
Figure 2. PET CT showing a sigmoid colon tumour on the left.
DISCUSSION
Procalcitonin (PCT) importance: procalcitonin is primarily recognised for its role in the body’s response to bacterial infections, where its levels rise significantly, aiding in the differentiation of bacterial aetiologies and guiding antibiotic therapy[3]. However, its relevance extends beyond infections. In the setting of MTC, elevated PCT levels serve as a valuable biomarker. Unlike calcitonin, which can be unstable and vary significantly between assays, PCT provides a more reliable measure due to its stability and consistent assay results[4]. Persistent elevation of PCT above 2 ng/ml, which can reach up to 1,000 ng/ml despite resolving infection, warrants further investigation for MTC[5]. This makes PCT a crucial biomarker for the early detection and continuous monitoring of MTC. Regular monitoring of PCT levels can offer insights into the prognosis of MTC patients; a decline in PCT post-treatment suggests a positive therapeutic response, whereas rising levels may indicate recurrence or progression[6]. This utility underscores the need for integrating PCT measurements into routine clinical practice for MTC patients, enhancing the ability to detect recurrences early and tailor treatment strategies accordingly.
CEA: Our patient presented with early-stage sigmoid cancer, which typically does not result in significantly elevated CEA levels. In the early stages of sigmoid cancer, CEA levels may be slightly elevated but often remain within the normal range or just above it[7]. Additionally, our patient had normal CA19-9 levels, which increase in cases of advanced or severe sigmoid cancer[8]. However, our patient exhibited a CEA level of 69.29 ng/ml. This elevated CEA level supports the possibility that CEA can also be elevated in MTC. In MTC, CEA becomes particularly prominent when tumour cells dedifferentiate and lose their ability to produce calcitonin[9]. In such scenarios, CEA levels remain a reliable indicator of disease status, making it a critical biomarker for monitoring MTC progression and response to treatment.
CONCLUSION
In conclusion, this case underscores the critical role of PCT and CEA in the diagnosis and monitoring of MTC. Persistent elevation of PCT levels post-infection, coupled with significant CEA levels, can aid in the early detection and management of MTC. These biomarkers provide reliable measures for assessing disease status and therapeutic response. While the current findings highlight their utility in clinical practice, further studies are needed to explore their full potential and establish standardised guidelines for their use in MTC management.