ABSTRACT
Immunoglobulin G4-related disease (IgG4-RD) is an autoimmune disease characterized by elevated serum IgG4 levels. It has the potential to affect multiple organs. Despite the diverse manifestations of IgG4-RD, the association with coronary artery disease (CAD) remains poorly understood due to limited evidence. We report the case of a 52-year-old male patient who exhibited typical angina upon exertion, accompanied by elevated serum IgG4 levels. Coronary computed tomographic angiography (CCTA) revealed the presence of pseudotumor formations surrounding and aneurysm changes affecting all coronary arteries, consistent with IgG4-RD. The patient was treated with prednisolone and azathioprine, with the possibility of additional rituximab therapy if symptomatology failed to improve. This case sheds light on the rare occurrence of IgG4-RD with coronary artery involvement and underscores the importance of recognizing this unique clinical entity for appropriate management and further research.
LEARNING POINTS
- Immunoglobulin G4-related disease (IgG4-RD) is a chronic systemic disease characterized by inflammatory fibrosis and high serum IgG4 levels.
- IgG4-RD can involve the coronary artery, presenting as a coronary aneurysm, and may mimic coronary artery disease.
- Treatment of IgG4-RD with coronary artery involvement includes corticosteroid therapy, with or without other immunosuppressant, as well as surgical intervention.
KEYWORDS
Coronary aneurysm, coronary artery disease, immunoglobulin G4-related disease, pseudotumor
INTRODUCTION
Immunoglobulin G4-related disease (IgG4-RD) is an immunologic fibro-inflammatory systemic disease with the potential to manifest in various organ systems[1]. Its manifestations can include autoimmune pancreatitis, Mikulicz’s disease affecting the lacrimal gland, retroperitoneal fibrosis, aortic aneurysm, aortitis, and constrictive pericarditis[2]. Depending on the affected organ, patients with IgG4-RD can present with diverse symptoms. Complications can include obstruction or compression due to organomegaly or dysfunction caused by cellular infiltration or fibrosis. In this case report, we present a unique instance of IgG4-related pseudotumor encasing the coronary arteries.
CASE REPORT
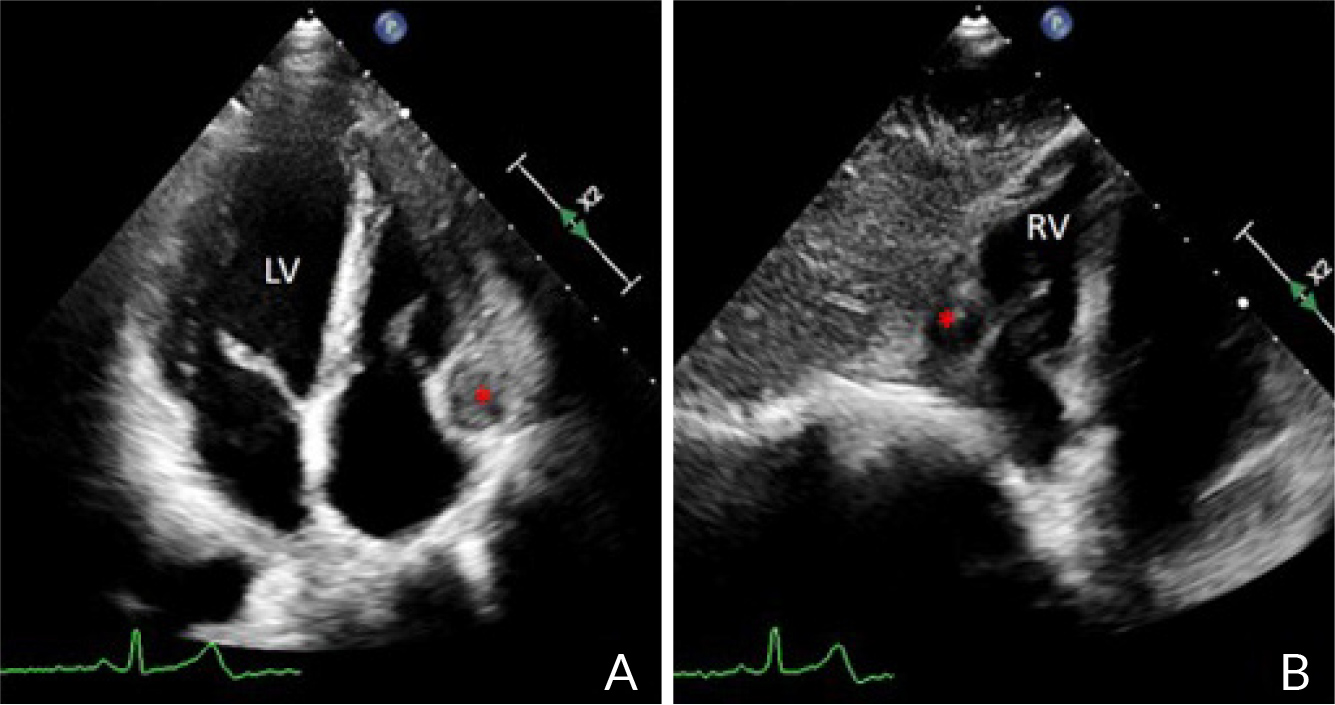
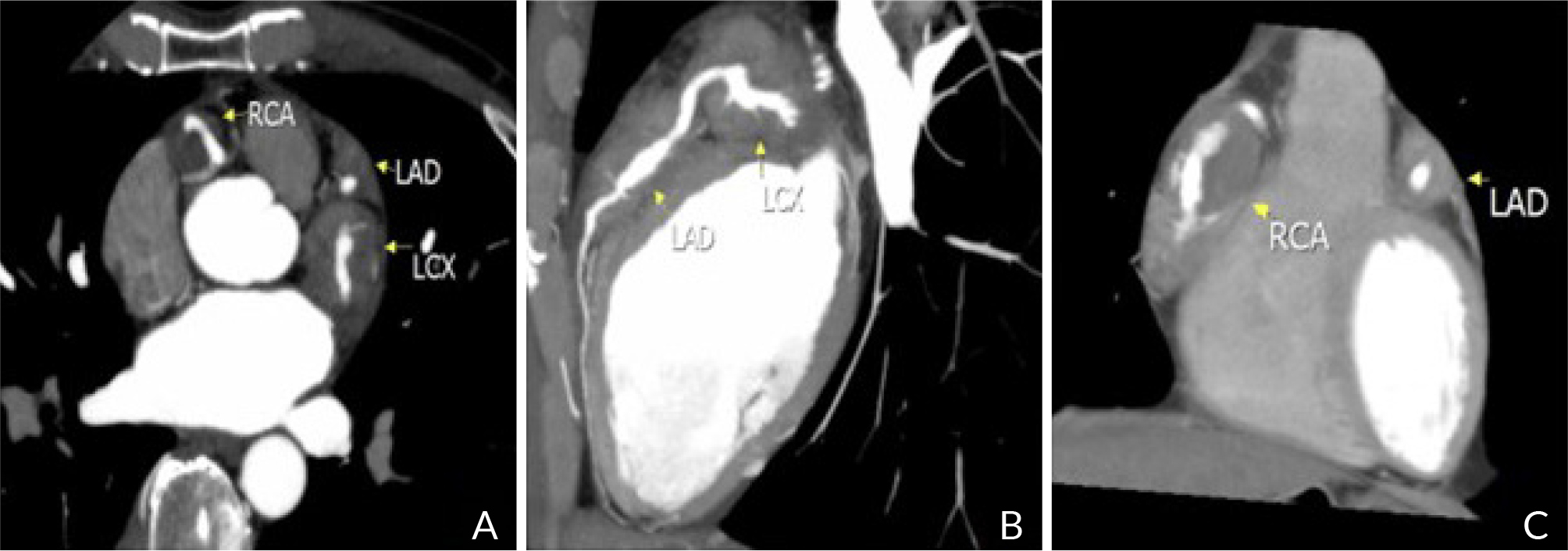
We present a case of a 52-year-old man who initially presented with swelling of the lacrimal and salivary glands. A diagnosis of possible IgG4-RD was made based on markedly elevated serum IgG4 levels (2,560 mg/dl) and characteristic lymphoepithelial sialadenitis on salivary gland pathology. Effective control of the disease was achieved with low-dose prednisolone. However, in 2021, the patient experienced a new onset of typical angina and sought medical attention at the emergency department of Burapha University Hospital. He denied any family history of coronary artery disease (CAD), as well as tobacco or illicit drug use. The electrocardiogram showed a sinus rhythm without ST segment abnormality. A chest X-ray and other laboratory findings, including cardiac troponin levels, were unremarkable. Transthoracic echocardiogram revealed a tubular structure located at the atrioventricular groove (Fig. 1), suggesting a possible dilated coronary artery or surrounding mass. Subsequent coronary computed tomographic angiography (CCTA) confirmed the presence of a multilobulated hypervascular mass encasing all three coronary arteries (Fig. 2 and 3), causing alternating enlargements, aneurysms, and occlusion at the proximal left circumflex artery (Fig. 4). Additionally, CCTA revealed evidence of enlarged mediastinal nodes and extra-pleural nodes at right paravertebral regions. Considering all these findings along with a history of IgG4-RD, the patient consulted with a rheumatologist, leading to a provisional diagnosis of IgG4-RD with coronary artery involvement.
(click to enlarge)
Figure 1. Transthoracic 2-dimensional echocardiogram (A: apical-4 chamber view, B: subcostal view) showed a tubular structure, measuring 28 x 22 mm (asterisk), located at the atrioventricular groove. LV: left ventricle; RV: right ventricle.
(click to enlarge)
Figure 2. Coronary computed tomographic angiography with maximum intensity projection reconstructions (A: axial image, B: sagittal image, C: coronal image) showed pseudotumor formation (arrow) around the coronary arteries. LAD: left anterior descending artery; RCA: right coronary artery; LCX: left circumflex artery.
(click to enlarge)
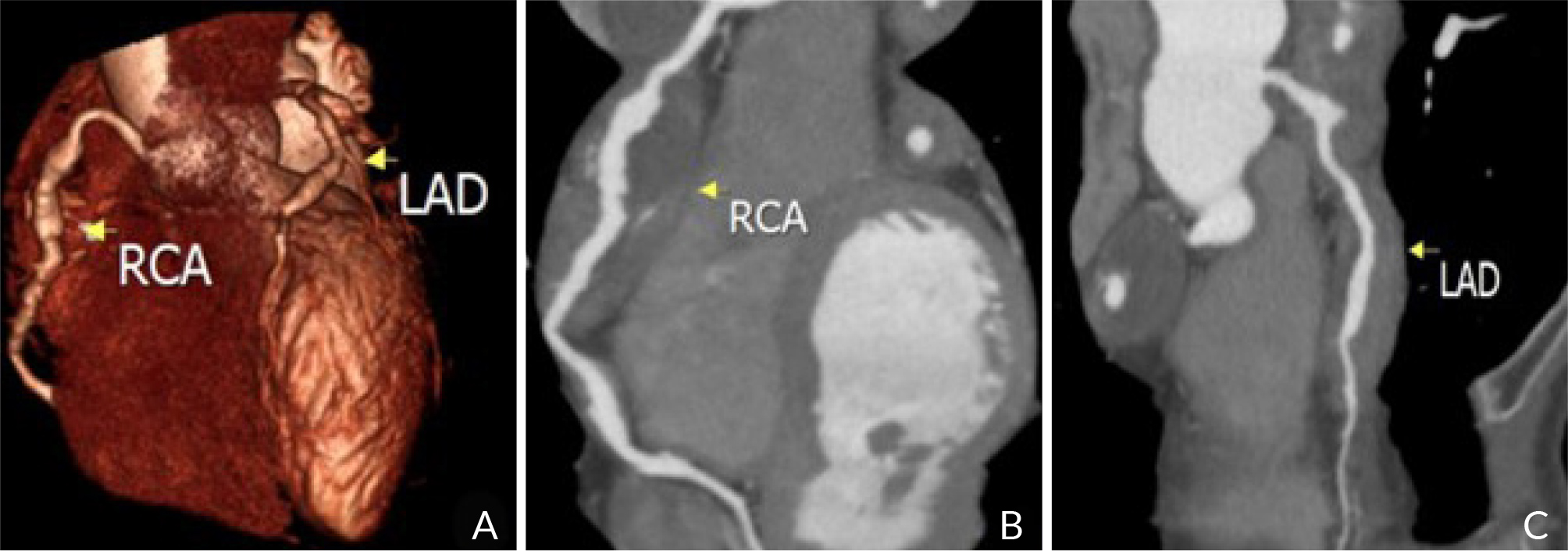
Figure 3. Coronary computed tomographic angiography. (A) Volume rendering image showed aneurysmal change of RCA and LAD. (B) curved multiplanar reconstruction of the RCA showed aneurysmal change and pseudotumor formation (arrow) around the artery. (C) Curved multiplanar reconstruction of the LAD showed aneurysmal change and pseudotumor formation (arrow) around the artery. LAD: left anterior descending artery; RCA: right coronary artery.
(click to enlarge)
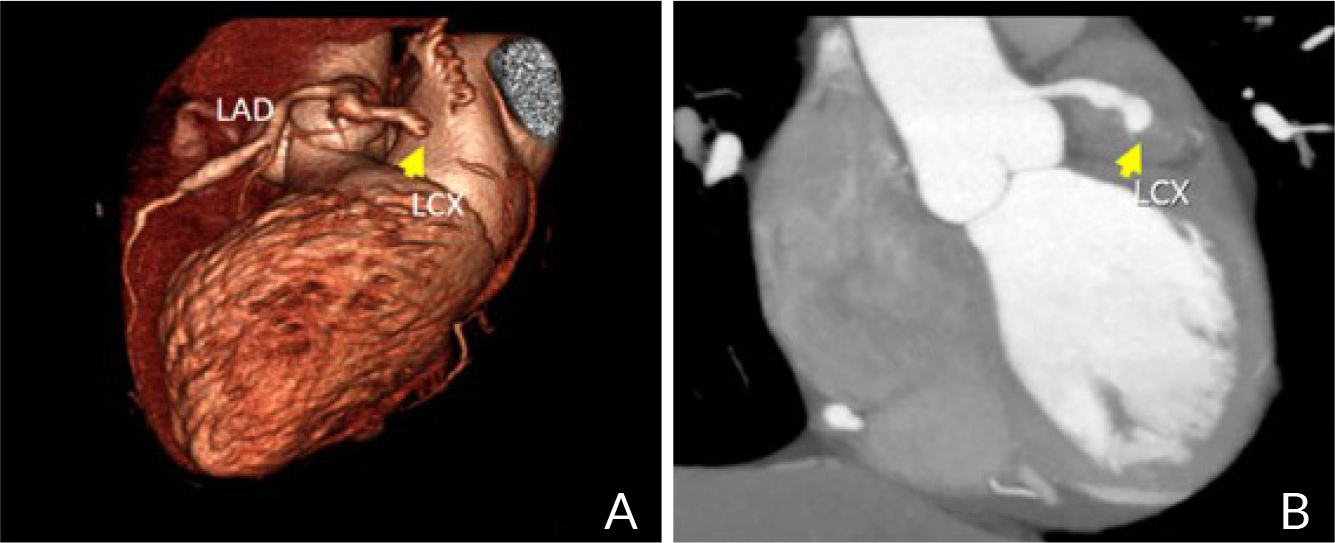
Figure 4. Coronary computed tomographic angiography (A: volume rendering image, B: maximum intensity projection reconstruction coronal image) showed occlusion of the proximal part of LCX (arrow). LAD: left anterior descending artery; LCX: left circumflex artery.
The patient received treatment with prednisolone and azathioprine prescribed by the rheumatologist, while the cardiologist prescribed aspirin, atorvastatin, and long-acting nitrate. After two months of treatment, the patient’s serum IgG-4 levels decreased to 1,460 mg/dl; however, he did not report improved chest pain including during vigorous exercise. Consequently, we conducted a coronary angiography and performed a percutaneous coronary intervention. The angiography revealed a chronic total occlusion at the proximal part of the left circumflex artery and aneurysmal changes in all vessels. Unfortunately, the interventional cardiologist faced challenges passing the wire directly to the lesion. Ultimately, the decision was made to prescribe warfarin for coronary artery aneurysm treatment. During discussions with the rheumatologist, rituximab was considered as part of the induction therapy in case the patient’s symptoms progressed.
DISCUSSION
Coronary artery involvement in IgG4-RD was first described in 2008 by Matsumoto et al.[3], who demonstrated a tumefactive lesion surrounding the mid part of the right coronary artery and elevated IgG4 levels. Coronary involvement in IgG4-RD has been scarcely reported in the literature[4], and myocardial ischemia as its presenting feature is even rarer[5]. Among the 15 previously reported cases of IgG4-RD[6], patients diagnosed with CAD also exhibited features such as thickening of coronary artery walls, surrounding soft tissue, and giant coronary artery aneurysms, which matched our case.
The present case of IgG4-RD involving CAD was not diagnosed based on tissue biopsy, which is a useful tool for diagnosing IgG4-RD, but rather on the findings of heterogeneous pseudotumor formation around the coronary arteries and aneurysmal changes on CCTA. Additionally, serum IgG4 levels were found to be very high (2,560 mg/dl). Therefore, IgG4-RD was diagnosed, even without a tissue biopsy from the coronary vessels. According to the 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD[7], this patient can be classified as a possible case of IgG4-RD. The periarterial thickening and luminal stenosis of the proximal part of the left circumflex artery caused the patient’s chest pain during vigorous exercise.
Corticosteroids are the first-line treatment in IgG4-RD[4] and have shown effectiveness in patients with coronary pseudotumors[8]. Azathioprine is frequently used in immune-mediated diseases. According to consensus guidance, azathioprine might be initiated as a prednisolone sparing therapy in IgG4-RD[9]. However, the efficacy of azathioprine in IgG4-RD remains unclear as it appears to be effective in only a minority of cases with pancreatic involvement.
The pathogenesis of IgG4-RD is unclear but may involve the humoral immune system[10], as these patients have increased IgG4 levels and show a good response to rituximab treatment (B-cell depletion treatment). Rituximab should offer an effective induction therapy for these patients.
CONCLUSION
IgG4-RD should be considered in the differential diagnosis of any patient with tumefactive lesions surrounding the coronary arteries, as it can present as CAD. The measurement of serum IgG4 levels and CCTA may be useful for diagnosis and monitoring of the disease. The choice of treatment was based on recommendations and the experience of the prescribing rheumatologists.