(click to enlarge)
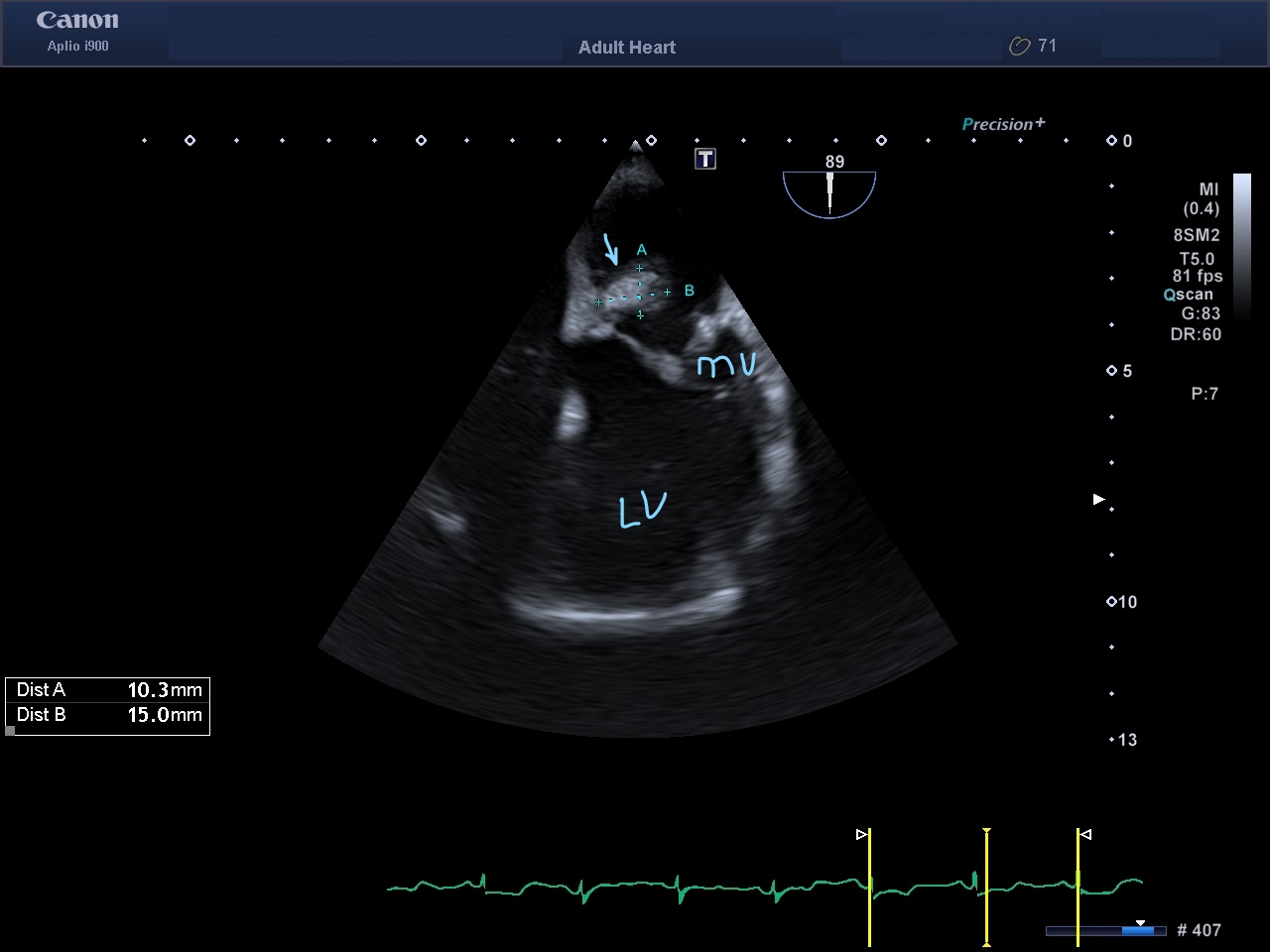
Figure 1. Transoesophageal echocardiography, mid-oesophageal view: arrow, the posterior annular mass; LV, left ventricle; MV, mitral valve; LA, left atrium.
Mitral annulus calcification is a common incidental finding in echocardiography examination of predisposed populations. On the other hand, caseous calcification of the mitral annulus is a rare variant that challenges the physician to differentiate it from different causes of cardiac masses. We describe a case of incidentally discovered caseous calcification confirmed with CT cardiac and cardiac magnetic resonance.
Echocardiography, cardiac mass, mitral annular calcification
The main feature of mitral annular calcification is progressive calcium deposits, involving the mitral valve fibrous annulus[1]. It is diagnosed incidentally by echocardiography, as it appears as a highly echogenic, irregular structure involving the annulus of the mitral valve close to the posterior atrial ventricular groove, and is associated with acoustic shadowing[1]. Usually, the mitral valve leaflets and chordae tendineae are spared. Calcification may progress in the sub-valvular area in more severe cases, beneath the posterior leaflet, and encroach on the leaflet and into the myocardial wall. This might lead to left ventricle inflow obstruction[2]. The calcific mitral inflow stenosis is at the level of the mitral annulus, with relative sparing of the leaflet tips. Another rare complication is producing a smooth, round penannular mass that is less echodense than typical mitral annular calcification, mimicking tumours, abscesses or thrombi, as in the current case report.
The patient was a 64-year-old woman known to have had diabetes for 15 years, for which she was taking oral hypoglycaemic agents, hypertension for 10 years and was a non-smoker. The patient was referred from a medical outpatient clinic for evaluation of non-specific chest pain and normal ECG. She was seen in an echocardiography clinic. BP was 130.60 mmHg, heart rate 74/minute; she was afebrile. The physical examination was normal, and there was no heart murmur. Renal function was normal. Echocardiography (transthoracic followed by transoesophageal) (Fig. 1) showed normal left and right ventricle size and systolic function with mild mitral regurgitation. There was a heterogeneously echogenic mass in the posteromedial part of the mitral annulus with significant projection into the left atrium (Fig. 1, Video 1). There was mild mitral regurgitation but no inflow stenosis. Mild aortic sclerosis had no regurgitation or stenosis. As the patient had no signs of sepsis, endocarditis and abscesses were ruled out. The remaining differential diagnosis was between cardiac tumour and caseous mitral annulus calcification. We proceeded with cardiac magnetic resonance (CMR) (Fig. 2 and 3), which showed a well-defined, thin rim enhancement (suggesting fibrotic reaction) and centrally non-enhancing mass (suggesting an avascular nature) seen in the posteroinferior left atrium in close relation with the posterior mitral annulus and posterior mitral leaflet. The correlation with cardiac CT (Fig. 4 and 5) showed the following. A well-defined mass with central soft calcific density and peripheral dense nodular calcification was noted in the posterior mitral annulus and adjacent myometrium, with projection into the left atrium. The mitral annulus calcification was in continuation with the mass. Therefore, combined MR and CT imaging features suggested a benign avascular calcified mass in the posterior mitral annulus and adjacent myometrium with projection into the left atrium. During the CT coronary examination using a 320-slice multi-detector computed tomography machine, coronary angiography was performed using prospective ECG gating; 90 mL of Omnipaque 350 was injected as IV contrast at a rate of 6 mL/s and 3D postprocessing was performed. Coronary findings: calcium Agatston score = 80, with normal coronaries. Non-coronary cardiac findings: A well-defined mass with central soft calcific density and peripheral dense nodular calcification was seen in the posterior mitral annulus and adjacent myometrium with projection into the left atrium. The mitral annulus calcification was in continuation with the mass. The pericardial contour was preserved with no effusion, thickening or calcification. A benign calcified mass in the posterior mitral annulus and adjacent myometrium with projection into the left atrium most likely represents caseous liquefication of posterior mitral annulus calcification. The patient was advised to have follow-up visits biannually and was reassured.
Mitral annulus calcification is a common degenerative disorder affecting cardiac fibrous supportive tissue. It occurs mostly in the older age group (>50 years), predominantly in women, and in hypertension and renal failure patients[3]. Early published data were from patients who were operated on, and the lesions were given different names (caseous ‘tumour’ of the mitral annulus, mitral annular calcification with central caseation and sterile, caseous mitral valve annular abscess, and tumour-like mild annular calcification with central liquefaction). They share a common histopathology: central liquefication necrosis that consists of calcium, fatty acids and cholesterol[3,4,5]. The incidence of caseous calcification of the mitral annulus varies between different reports. Caseation of the calcified ring was seen in seven hearts out of 258 (2.71%) autopsies of cases of mitral annulus calcification in a pathological clinical study[3]. In an echocardiographic screen of mitral annular calcification, 18 cases were identified and one in the tricuspid area, so a total of 19 were diagnosed with caseous calcification out of 3007 (0.63%) screened cases of annular calcification[6]. Three patients underwent mitral valve replacement and showed a solid mass adherent to the posterior portion of the mitral valve with a toothpaste-like, white caseous material in the middle. Three cases had caseous calcification among 9000 people from the general population examined by echocardiography over 1.5 years (<1%)[4]. Usually, the caseous calcification of the mitral annulus is asymptomatic and is detected incidentally by a transthoracic or transoesophageal echocardiogram for other reasons. It has been described in the literature as a sizeable mass on echocardiography that is rounded with an echodense patch in the periannular region of the mitral valve, and a clear central echo lucent zone[5,6,7]. The acoustic shadowing is absent behind the mass because of the absence of dense calcium deposits in mitral annular calcification. Early case reports misidentified caseous calcification as myocardial abscesses, which were surgically removed[3]. Sometimes a misdiagnosis as a tumour might lead to unnecessary exposure to explorative cardiotomy[3]. Caseous calcification is usually a benign condition of a dynamic process[8,9,10]. In a follow-up of 14 cases of caseous calcification in the prospective echocardiographic study by Deluca et al., it was found that three patients with mitral annulus calcification progressed to caseous calcification, and three patients with caseous calcification reverted to mitral annulus calcification during the study period[8]. There was a reported case of caseous calcification with spontaneous resolution in a 60-year-old woman[9]. Another case report found a partial capsule rupture, including mobile remnants at the point of rupture with spontaneous resolution in asymptomatic patients[10]. Based on these reports and the absence of consensus in managing caseous calcification, we opted for only a follow-up of our patient. CT helps to diagnose caseous calcification and differentiates it from other kinds of cardiac masses. On CT, caseous calcification is identified as a non-contrast-enhancing hyperdense mass that is well-defined, oval or crescent-shaped, surrounded by dense calcification. The mass is usually present in the posterior mitral annulus[11]. CMR is another cardiac imaging modality that can help evaluate caseous calcification[4,6,11]. The caseous calcification appears n CMR as a well-defined mass with a hyperintense centre and hypointense rim on T1-weighted fast spin-echo imaging or T1-weighted spoiled gradient-echo imaging[8]. On T2-weighted imaging, caseous calcification appears as a mass without a central signal and with a high-intensity ring[8]. Characteristic features of caseous calcification on echocardiography, CT and CMR distinguish caseous calcification from myocardial abscesses, tumours or thrombi.
Caseous mitral annulus calcification is a form of mitral annulus calcification that can be incidentally discovered as a cardiac tumour. The combination of echocardiography, CMR and CT should differentiate it from other entities.
(click to enlarge)
Figure 1. Transoesophageal echocardiography, mid-oesophageal view: arrow, the posterior annular mass; LV, left ventricle; MV, mitral valve; LA, left atrium.
Video 1. Transoesophageal echocardiography
(click to enlarge)
Figure 2. Early gadolinium-enhanced image: arrow, the mass; LA, left atrium; LV, left ventricle

(click to enlarge)
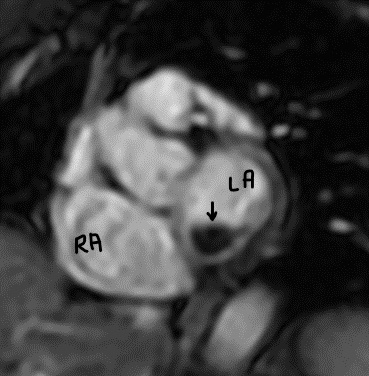
Figure 3. Late gadolinium-enhanced image: RA, right atrium; LA, left atrium; arrow, non-enhancing mass

(click to enlarge)
Figure 4. Contrast CT sagittal view: LA, left atrium; arrow, the mass; A, aorta

(click to enlarge)
Figure 5. Contrast cardiac CT: M, mass attached to posterior mitral annulus (arrows); RA, right atrium; LV, left ventricle; LA, left atrium