(click to enlarge)
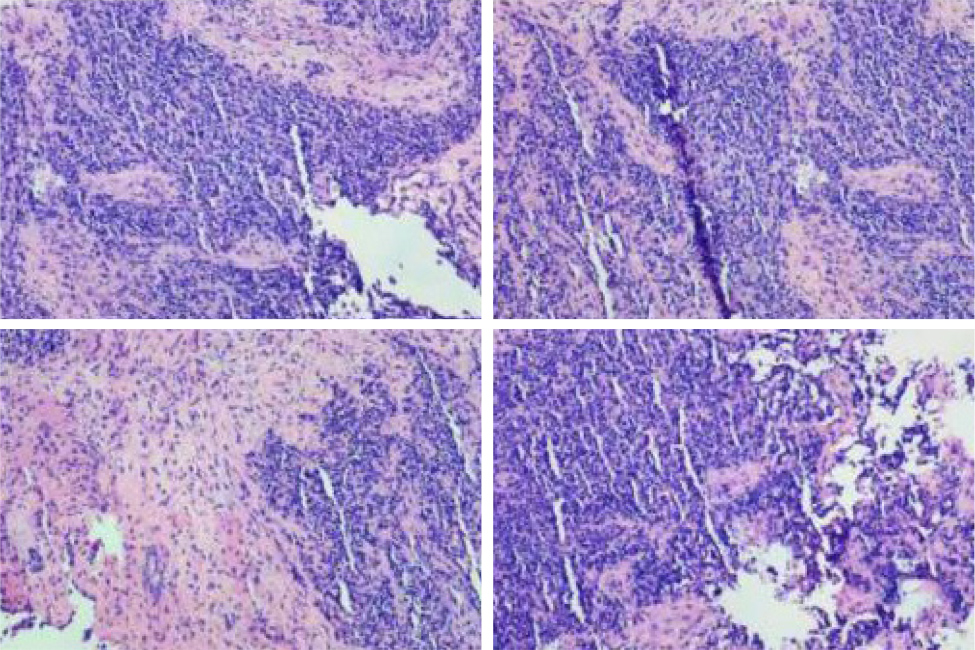
Figure 1. Immunohistochemistry (-), Vimentin (+), CD56 (3+): Ki-67 70%, S100 (-), CD117 (-), CK5/6 (-) P63 (-), NSE (-), CD99 (Suspicious+), HMB45 (-), Syn (-), CgA (-)
Introduction: Rhabdomyosarcoma is a high-grade malignant neoplasm with skeletal muscle differentiation; a common soft tissue sarcoma in children but considered one of the rarest in adults.
Case description: We report a case of 35-year-old male with a chronic productive cough and haemoptysis for five days. A CT scan of the nasopharynx revealed a blocked left maxillary and ethmoid sinus with bone destruction. These findings raised a suspicion of a tumour, and trans-nasal endoscopic sinus surgery was performed.
Discussion: Nasal rhabdomyosarcoma is a rare adult malignant tumour. Most patients have lymphatic metastasis or skull base tumour infiltration at the time of the initial diagnosis and treatment, which poses a challenge to the diagnosis and management.
Conclusion: Nasal acinar rhabdomyosarcoma, one of the histopathological types of rhabdomyosarcoma, has rapid disease progression and high mortality. Therefore, the treatment of rhabdomyosarcoma requires a combination of surgery, chemotherapy, radiotherapy, and immunotherapy to work together to achieve the best care for the patient.
Rhabdomyosarcoma, endoscopic sinus surgery, acinar
The patient provided informed consent for this case report, and institutional review board approval from the primary care hospital was obtained.
A 35-year-old male presented with a history of cough and expectoration for three months, and haemoptysis for five days. The patient had no significant past or family history or any known allergies. After initial evaluation and based on the suggestive history, a presumptive diagnosis of bronchiectasis was made, and the patient was admitted to the respiratory department at our centre on 10 January 2019.
Imaging studies were performed soon after admission to confirm the diagnosis of bronchiectasis. A computerised tomography (CT) scan of the nasopharynx was also performed, and it showed a space-occupying lesion in the left maxillary sinus. Another space-occupying lesion was identified, filling the left ethmoid sinus with associated bone destruction. These findings raised suspicion of a tumour, and further investigation was planned. It was concluded that the best mode of analysing the lesions in the sinus cavities would be surgical resection and pathological examination. A left trans-nasal endoscopic sinus surgery with tumour resection was arranged for the next day.
Tumours in the left middle nasal meatus and ethmoid sinus were found during the surgery. The tissue in the ethmoid sinus showed fish-like changes and bone destruction extending to the skull base. To identify the histopathological type of the tumours, the pathology department requested a frozen section. The frozen section examination showed that the tumour from the left ethmoid sinus was suggestive of a malignant tumour, olfactory neuroblastoma. This impression led to complete resection of the tumours from the ethmoid and mandibular sinuses.
No intraoperative complications occurred, resulting in an uneventful surgery. The patient’s left nasal cavity was filled with an expanded sponge for haemostasis. A few days after the surgery the nasal packing was removed, and a repeat endoscopy was performed.
Histopathological examination results and immunohistochemistry showed an acinar type of rhabdomyosarcoma in the left maxillary sinus. Microscopic images of the region of interest in the tumour and the immunohistochemistry are shown in Figure 1.
On 22 January 2019 he was transferred to the Sun Yat-sen University Affiliated Cancer Hospital at Guangzhou for further treatment and received chemotherapy with Cyclophosphamide + Adriamycin + Vincristine (CAV). The patient was followed up for six months without complications.
The patient was diagnosed in January 2019 and died in October 2021.
Nasal rhabdomyosarcoma is a rare adult malignant tumour. It accounts for only 10–15% of head and neck rhabdomyosarcomas[1]. Most patients have lymphatic metastasis or skull base tumour infiltration at the time of initial diagnosis and treatment, which poses a challenge to the diagnosis and management. Imaging studies can arouse suspicion of this disease, but histopathology with immunohistochemistry is the only definitive diagnostic tool[2]. Nasal acinar rhabdomyosarcoma, one of the histopathological types of rhabdomyosarcoma, has rapid disease progression and high mortality. Therefore, the treatment of rhabdomyosarcoma requires a combination of surgery, chemotherapy, radiotherapy and immunotherapy to work together to achieve the best care for the patients[3]. Surgical resection is usually the first step in managing rhabdomyosarcoma, followed by chemotherapy and/or other treatment modalities decided on a case-by-case basis. Regular follow-up and reassessment to ensure no recurrence are vital to its management[2]. The patients also usually need psychological care as well as rehabilitation.
Compared with the paediatric population, diagnosing rhabdomyosarcoma in adults is difficult as it is easy to miss, and there is a high probability of misdiagnosis, considering that this is a rare tumour in adults. This leads to a delay in diagnosis and treatment. It is well known that the prognosis of rhabdomyosarcoma is significantly poorer in adults than in children. The delay in diagnosis and treatment worsens the already low 5-year survival rates in adults[4]. The survival rate of many adult patients with rhabdomyosarcoma is two years or less.
The patient in our report was initially treated with surgical resection followed by chemotherapy at a different centre. In patients with rhabdomyosarcoma, the complexity of surgical resection depends on the site and size of the primary tumour. In our patient, endoscopic sinus surgery was believed to be the best technique to resect the tumour based on its site.
We followed a comprehensive protocol to ensure the patient received the best care possible.
(click to enlarge)
Figure 1. Immunohistochemistry (-), Vimentin (+), CD56 (3+): Ki-67 70%, S100 (-), CD117 (-), CK5/6 (-) P63 (-), NSE (-), CD99 (Suspicious+), HMB45 (-), Syn (-), CgA (-)