ABSTRACT
COVID-19 vaccines were introduced soon after the COVID-19 pandemic emerged in 2020. Various side effects were reported worldwide, including several types of common systemic side effects such as fever and general fatigue. Reports of other rare manifestations also emerged. We report the case of an adult male with a rare systemic syndrome mimicking lymphoma after he had received the first dose of an mRNA-based COVID-19 vaccine. After nearly 6 months of investigation with suspicion for an infection or malignancy, all symptoms resolved, laboratory tests normalized, and imaging showed no sign of active disease.
LEARNING POINTS
- A lymphoma-like reaction is a possible side effect of COVID-19 vaccination.
- It is important to rule out other causes of systemic symptoms before diagnosing a reaction to a COVID-19 vaccine.
- A lymphoma-like reaction following administration of a COVID-19 vaccine has a good prognosis.
KEYWORDS
SARS-CoV-2, COVID-19 vaccine, lymphoma-like reaction
CASE DESCRIPTION
A 46-year-old Israeli man, with a medical history of testicular seminoma, was admitted to hospital due to a 10-day history of 40°C fever with shivering. A month before hospitalization, he had been vaccinated with a first dose of the Pfizer BNT162b2 COVID-19 vaccine. A few days later, he started experiencing night sweats, and during the following month had a slight weight loss of 4 kg and also experienced back pain which resolved following treatment with non-steroidal anti-inflammatory drugs (NSAIDS) and paracetamol. Upon admission, he complained of 6 days of dry cough. Physical examination revealed an enlarged spleen and enlarged inguinal and subclavian lymph nodes. Laboratory investigations including blood tests showed leucocytosis (16 K/µl) with neutrophilia (14.7 K/µl) and lymphopenia (0.7 K/µl), normocytic normochromic anaemia (9.4 g/dl), mild cholestatic elevated liver enzymes (alkaline phosphatase 200 U/l, gamma-glutamyl transferase 230 U/l) and elevated C-reactive protein (CRP) of 15 mg/dl and erythrocyte sedimentation rate (ESR) of 121 mm/1hr. A urine test was normal. A chest x-ray was normal, and an electrocardiogram showed inverted T waves in leads III and aVF. Fundoscopy showed a cotton wool spot in the right eye. A PCR test for COVID-19 was negative, and a COVID-19 anti-N protein IgG test showed levels of 86 AU/ml, implying non-immunity. An infectious panel including serological blood tests for Q fever, Brucella, cat scratch disease, Borrelia, Rickettsia, syphilis, mycoplasma, toxoplasma, leptospirosis, Epstein-Barr virus (EBV), cytomegalovirus (CMV), human immunodeficiency virus (HIV), hepatitis B and hepatitis C was negative. Cryptococcal antigen was negative in the blood. An autoimmune serology blood panel including antinuclear antibodies, anti-double-stranded deoxyribonucleic acid antibodies, anti-proteinase 3 antibodies, anti-myeloperoxidase antibodies, anti-glomerular basement membrane antibodies, liver-kidney antibodies, mitochondrial pyruvate dehydrogenase antibodies, and a connective tissue disease screen were all negative. Tests for coeliac disease including transglutaminase IgA and endomysial antibodies were negative. Tests for multiple myeloma including immunoglobulins and the kappa-to-lambda ratio and immunofixation were normal. In light of the patient’s medical history, cancer markers including beta human chorionic gonadotropin and alfa fetoprotein were checked and were negative. Screening for malignancy included positron emission tomography computed tomography (PET-CT) which showed pathological fluorodeoxyglucose (FDG) uptake in a sub-clavicular lymph node, retroperitoneal lymph nodes, and in the bone marrow, as well as an enlarged spleen and liver (Fig. 1). A fine needle biopsy from the sub-clavicular lymph node showed an atypical lymphoid infiltrate (Fig. 2). A bone marrow biopsy revealed a hypercellular bone marrow with over 10% of hyper-granular myeloid blasts with no signs of haemophagocytic lymphohistiocytosis (HLH) (Fig. 3). Fluorescence-activated cell sorting (FACS) showed no blasts and no chromosomal translocation of 15:17. The patient underwent abdominal magnetic resonance imaging (MRI) to locate an accessible lymph node for excisional biopsy, but none were found.

Figure 1 (click to enlarge)

Figure 2 (click to enlarge)
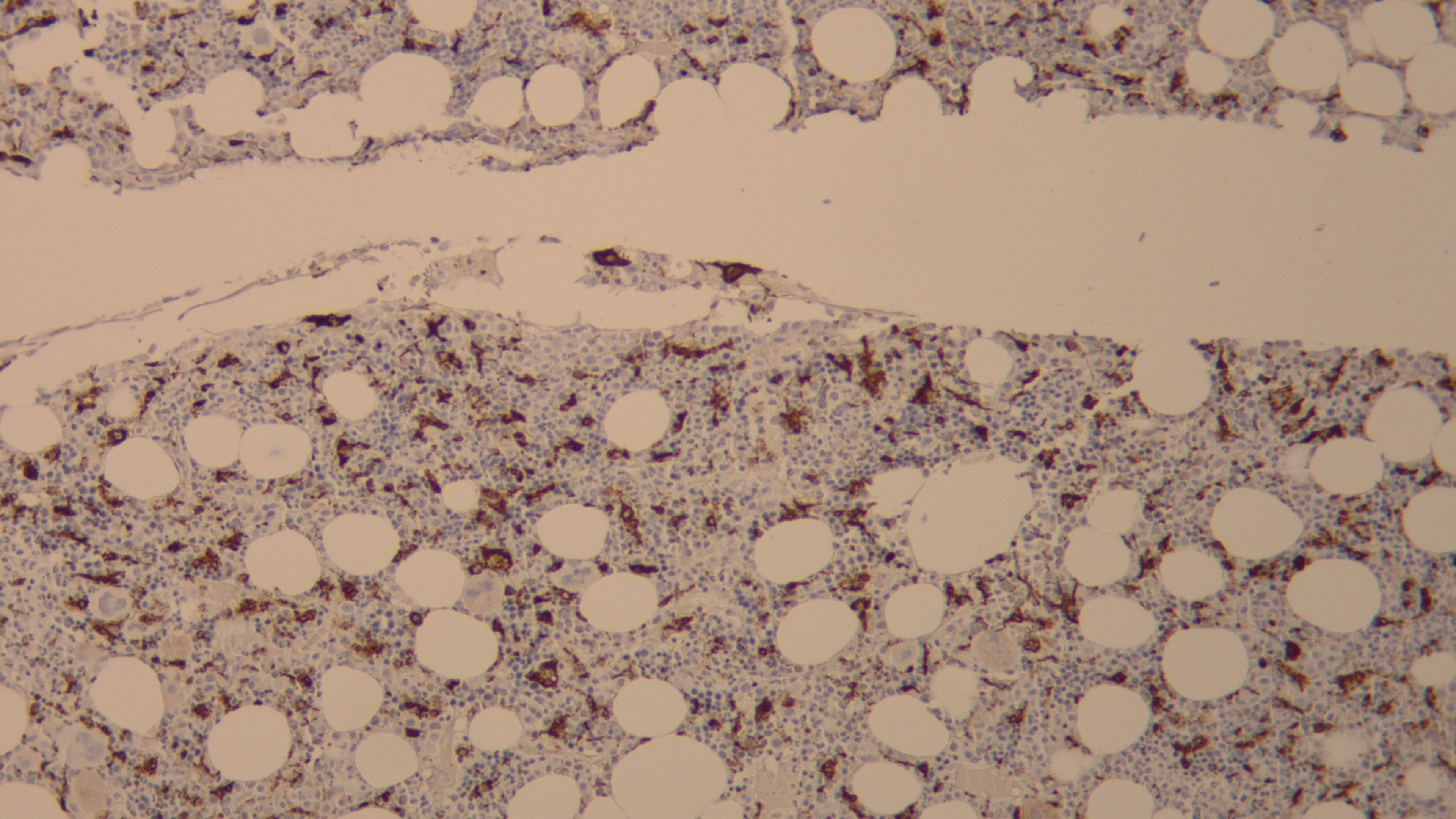
Figure 3 (click to enlarge)
Figure 1. PET-CT scan, performed as part of the initial investigation for malignancy, showing FDG uptake in a sub-clavicular lymph node.
Figure 2. A fine needle biopsy from a sub-clavicular lymph node with CD20 immunohistochemical staining showing an atypical infiltrate with high positivity for CD20 staining.
Figure 3. A bone marrow biopsy with positivity for CD68 immunohistochemical staining.
A month after the first bone marrow biopsy, a second bone marrow biopsy showed a single nodule of small lymphocytes. The patient also reported gradual relief of symptoms. Five months after first PET-CT scan, a second PET-CT scan showed resolution of findings, with no FDG uptake in any lymph node. Laboratory tests had also normalized, anaemia had resolved, and inflammatory marker levels had decreased to minimum levels.
DISCUSSION
The patient presented with prolonged systemic symptoms and lymphadenopathy, with a suspected diagnosis of low-grade lymphoma. He underwent a thorough investigation which revealed no evidence of cryptogenic infection or malignancy. Three months after symptom development, imaging and bone marrow biopsy findings had normalized. The patient’s symptoms could have been due to an immune-mediated reaction to the vaccine since they began soon after he had received the first dose of the Pfizer BNT162b2 vaccine for COVID-19, no other diagnosis was made and findings resolved. However, the patient presented with fever of unknown origin (FUO), and although up to 50% of patients with FUO remain undiagnosed even after a comprehensive investigation[1], in this case findings suggesting lymphoproliferative disease requiring further investigation.
Many different side effects and immune-mediated reactions following COVID-19 vaccination have been reported. Although several concurrent systemic side effects have been described, their combination was not determined to be a signature syndrome. Systemic symptoms were noted in about 50% of patients, but most were transient without significant sequelae. Fever, and especially high grade fever, was not prevalent[2,3].
There have been reports of ipsilateral lymphadenopathy following vaccination. A few studies described difficulty distinguishing between progression or signs of malignant disease and a reaction to the vaccine[4–6]. The National Comprehensive Cancer Network (NCCN) recommends delaying cancer patients' follow-up imaging studies for 4–6 weeks after completion of vaccination if possible. It is recommended that breast cancer patients receive the vaccine in the contra-lateral arm to the initial site of the tumour to prevent confusion and additional unnecessary biopsies[7,8]. Our patient had a history of testicular cancer, and therefore underwent a PET-CT scan for further evaluation of a relapse, 4 weeks after he had received the first dose of the vaccine. Pathology results from an enlarged lymph node in this patient showed atypical lymphoid hyperplasia, which can suggest malignancy or reactive hyperplasia caused by infection or an autoimmune disease[9]. Immunohistochemical tests did not demonstrate signs of malignancy, and typical chromosomal aberrations were not found. At this point the symptoms and imaging findings suggested an FUO with an undiagnosed source, on the assumption that the FUO occurring after vaccination was incidental. However, biopsy of the bone marrow showed dysplastic changes.
There are case reports of HLH after COVID-19 vaccination. Fever and lymphadenopathy suggesting lymphoma developed in a young woman 1 week after she had received the Moderna Spikevax vaccine. She was eventually diagnosed with post-vaccination reactive lymphadenitis and secondary HLH[10]. A few similar reports of systemic symptoms with lymphadenopathy with the same diagnosis following vaccination have been published. All patients recovered without serious sequelae[11,12]. A bone marrow sample in our patient showed no signs of HLH, although CD68 staining was positive throughout the specimen, highlighting multiple reactive histiocytes. There was a lymphocytic infiltrate rich in B cells which was suspicious for bone marrow lymphoma. However, flow cytometry testing was inconclusive for the diagnosis.
Kikuchi-Fujimoto disease (KFD) is another systemic syndrome which also mimics lymphoma and has been observed after COVID-19 vaccination. Four cases have been described in the literature, in two women and two men, aged 18–38 years. Three of the patients developed KFD after receiving only the first dose of the vaccine, while the other developed KFD after the second dose. All of the patients had a good prognosis with resolution of symptoms[13–15]. There have been sporadic reports of cases of KFD following administration of the influenza vaccine, the human papilloma virus vaccine and the Japanese encephalitis vaccine[16,17], although none of these are mRNA vaccines. Our patient's lymph node pathology was not consistent with KFD, as it lacked necrotic features, although KFD is a misleading pathological diagnosis.
In conclusion, reports are emerging of lymphoma-like reactions after COVID-19 vaccination. The described case is an example of an immune reaction to the vaccine, mimicking lymphoma without HLH, with a hypercellular bone marrow.