ABSTRACT
Intracranial neurenteric cysts are rare congenital lesions that can be mistaken for other lesions. They may contain mucous or serous glands, smooth muscle, lymphoid tissue and components of connective tissue. We report a case of neurenteric cyst which was detected accidentally by diagnostic imaging in the context of a thalamus infarct in a 45-year-old woman. We also discuss the results of a brief literature review and the pathological findings, imaging spectrum, evaluation and management of neurenteric cysts and thalamic infarctions.
LEARNING POINTS
- Neurenteric cysts are a rare type of foregut duplication cyst that are classified as intracranial or spinal and are associated with central nervous system abnormalities.
- Neurenteric cysts are usually benign and slow-growing, so conservative treatment can be provided if there are no symptoms.
- Thalamic stroke may be caused by arterial or venous infarction.
- Cardioembolism is the most common cause of thalamus infarction; variations in blood supply to the thalamus should be investigated in affected patients.
KEYWORDS
Acute cerebral infarction, central nervous system, endodermal cyst, intracranial cyst, neurenteric cyst
INTRODUCTION
Neurenteric cysts are rare congenital cysts of the central nervous system. Intracranial neurenteric cysts are very uncommon, being approximately three times less frequent than spinal neurenteric cysts. Fewer than 60 intracranial neurenteric cysts have been reported in the literature. Most are found in the posterior fossa, although rare supratentorial cysts have been described. We report a case of intracranial neurenteric cyst without other associated malformations, which was detected accidentally by diagnostic imaging in the context of cerebral infarction [1, 2].
CASE DESCRIPTION
A 45-year-old woman presented to the emergency department with slight weakness on her left side. She had a mild headache, dizziness and blurred vision. Her body temperature was 36.8°C, blood pressure was 150/80 mmHg, heart rate was 85 beats/minute, and respiratory rate was 20–25 breaths/minute. She had a history of intermittent treatment for hypertension and hyperlipidaemia. Physical examination showed signs of localized nerve defects with mild weakness in the left limbs. There was mild anisocoria of her left pupil with a slightly bigger pupil and left-sided ptosis. Auscultation of her heart and lungs was unremarkable. Blood and urine test results were within normal limits.
Emergency computed tomography (CT) of the head showed a hypodense region in the right thalamus caused by a suspected acute infarction. CT also revealed a dense soft-tissue mass in front of and slightly to the left of the medullary bulb (Fig. 1). The patient underwent magnetic resonance imaging (MRI) to accurately diagnose and evaluate these lesions. MRI demonstrated an acute cerebral infarction in the right thalamus, which was confirmed on diffuse pulse sequencing (Fig. 2).
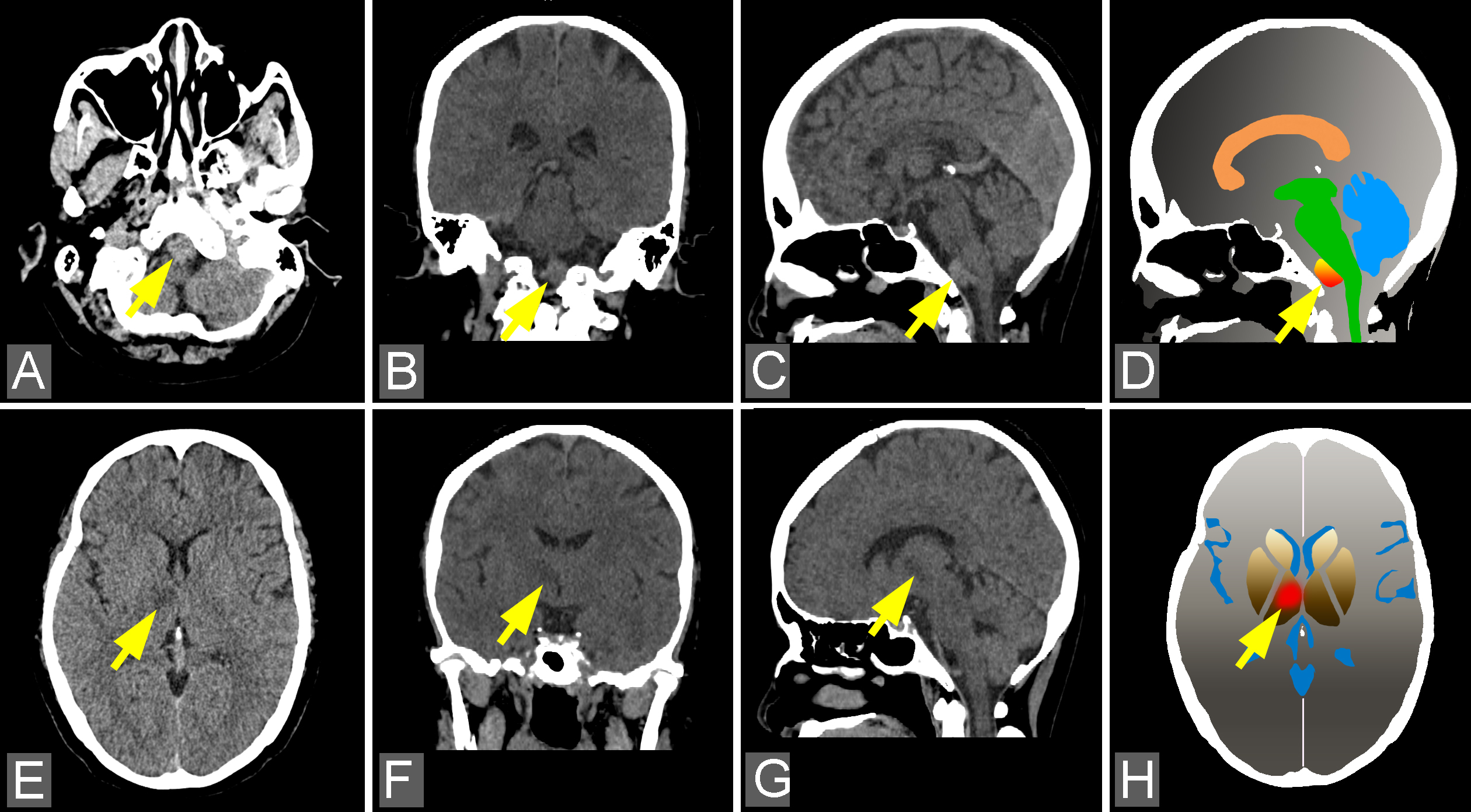
Figure 1 (click to enlarge)
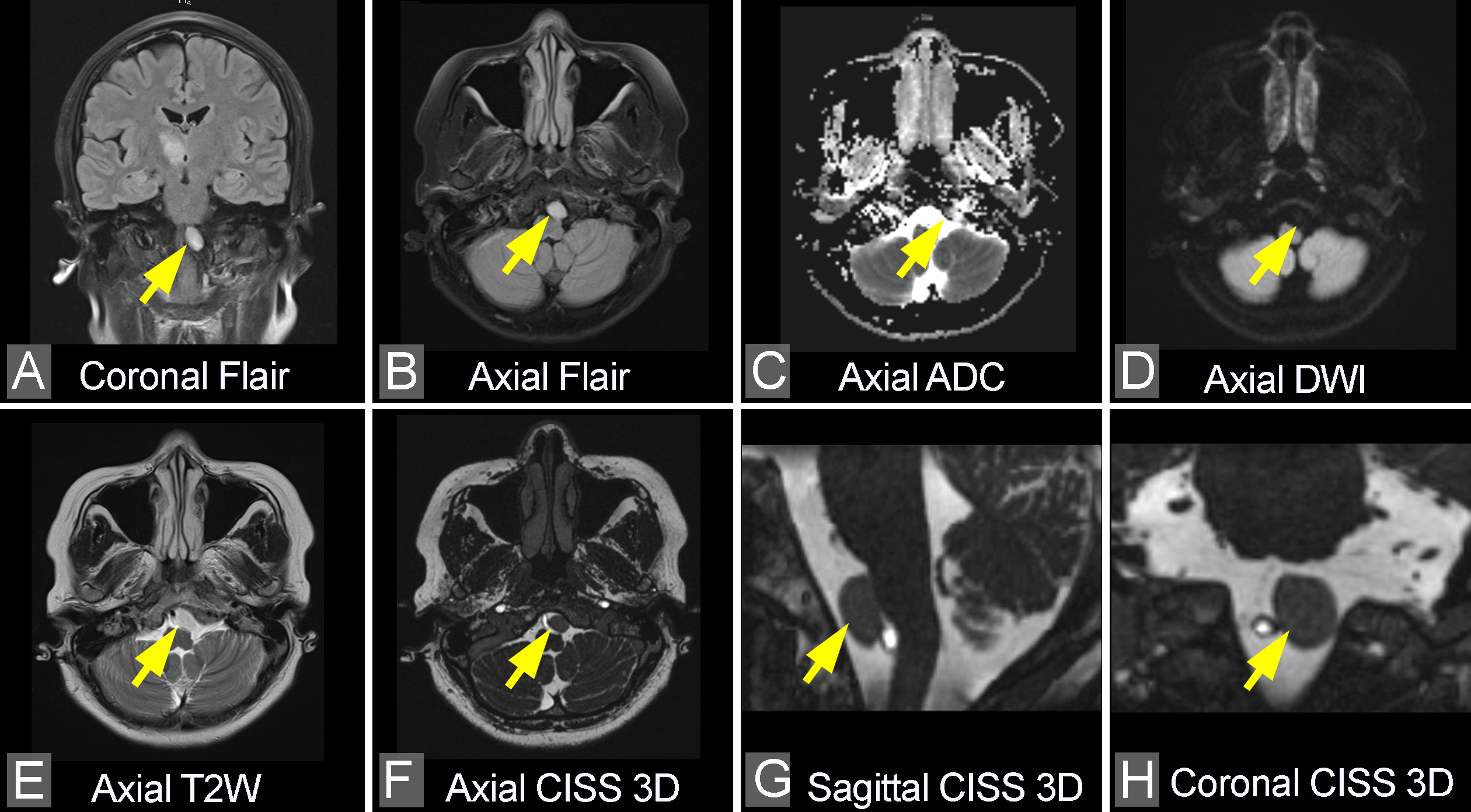
Figure 2 (click to enlarge)
Figure 1. CT images of the intracranial neurenteric cyst and a right-side thalamus infarct. (A) Axial, (B) coronal and (C) sagittal CT images showing a slightly hyperdense mass with well-circumscribed borders in front of and slightly to the left of the medullary bulb (arrows). (D) Diagram corresponding to (C). (E) Axial, (F) coronal and (G) sagittal CT images showing a hypodense region in the right thalamus (arrows). (H) Diagram corresponding to (E)
Figure 2. MRI of the neurenteric cyst adjacent to and slightly to the left of the medullary bulb, and measuring about 0.9×1.2×1.4 cm. (A) Coronal and (B) axial FLAIR images showing the hyperintense lesion. (C and D) Diffused images showing apparent diffusion coefficient (ADC) and diffusion weighted images (DWI) demonstrating unrestricted diffusion of the lesion. (E) On the axial T2W image, the neurenteric cyst shows a high intensity signal. (F, G and H) On CISS 3D images, the lesion has low signal intensity with sharply delineated borders (arrows)
MRI also showed a well-delineated lobulated cystic mass, identified as an intradural extramedullary lesion, in front of the medullary bulb and measuring about 0.9×1.2×1.4 cm. The signal intensity of the lesion was similar to white-matter intensity on T1-weighted images (T1W) and high-signal intensity on T2-weighted images (T2W). The adjacent medulla was displaced slightly dorsolaterally and was mildly flattened by the lesion, but the medullary signal was not affected (Fig. 3). The mass was not enhanced after administration of gadolinium contrast material (Fig. 4).
The patient was treated with prophylactic anticoagulant therapy and with hypertensive agents. She recovered and was discharged after 1 week. Her physical condition was almost normal at 5-month follow-up.
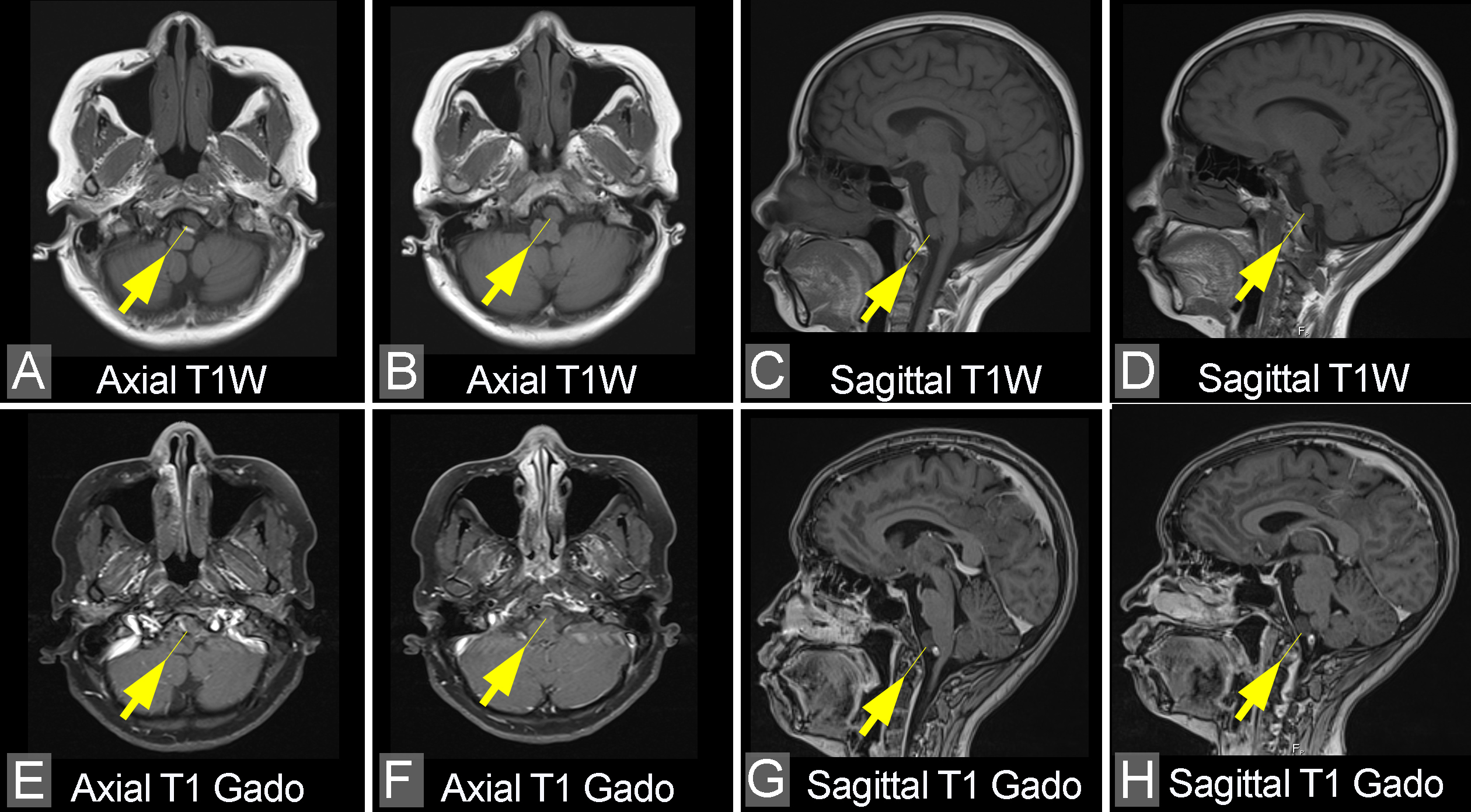
Figure 3 (click to enlarge)
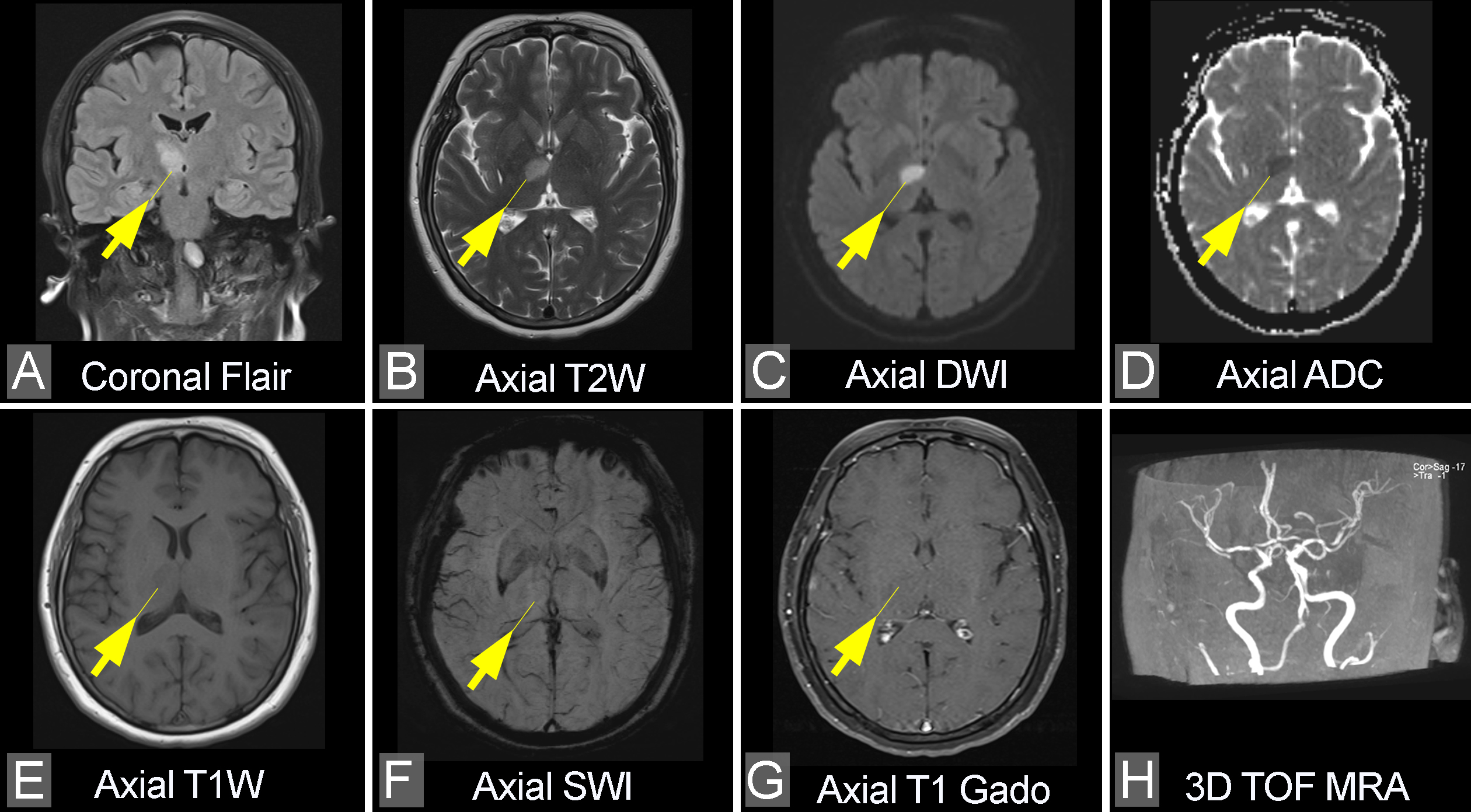
Figure 4 (click to enlarge)
Figure 3. (A–D) Non-contrast and (E–H) post-contrast T1W images demonstrate no enhancement of the lesion (arrows). The adjacent medullary bulb is very slightly compressed by the lesion and displaced dorsolaterally. No soft tissue or bony abnormalities are seen
Figure 4. MRI of the acute infarction in the right thalamus (arrows). (A) Coronal FLAIR and (B) axial T2W images show a lesion in the right thalamus with a hyperintense signal. (C) A hyperintense signal on diffusion weighted imaging (DWI) and (D) a hypointense signal on apparent diffusion coefficient (ADC) imaging indicate restricted diffusion. (E) Axial T1W image shows a slightly hypointense signal. (F) Susceptibility weighted imaging (SWI) shows no evidence of bleeding (note that small blood vessels can be observed in this image). (G) Axial postcontrast T1 image shows no enhancement of the lesion. (H) Reconstructed image of 3D time-of-flight (TOF) magnetic resonance angiography (MRA) shows normal main branches of the bilateral internal carotid artery
DISCUSSION
Neurenteric cysts are rare lesions of the central nervous system and account for 0.7–1.3% of all spinal cord tumours. They result from the inappropriate partitioning of the embryonic notochordal plate and presumptive endoderm during the 3rd week of embryonic life. They are more frequent in males. These cysts are commonly found in an intramural extramedullary compartment of the spinal canal, but a few are located in the intramedullary compartment. The neurenteric cyst in our case was in the extramedullary compartment and located in front of and to the left of the medulla, which is a very rare site [3].
Neurenteric cysts are often detected in the setting of spinal cord or cranial nerve compression. Our patient presented with left-sided paralysis caused by an acute right thalamus stroke and the neurenteric cyst was found accidentally. Neurological signs can be absent in patients with a solitary neurenteric cyst despite severe compression of the spinal cord. Consequently, neurenteric cysts in such patients are usually only identified following investigation by CT or MRI. MRI has many advantages over CT as it can directly visualize the lesion and any related cord changes. However, the associated bony abnormalities are better delineated on CT. Almost all of the neurenteric cyst is hypointense on T1W and isointense to hyperintense on T2W. Typically, the cysts rarely show rim enhancement by contrast medium [4].
The first-line treatment for neurenteric cysts is complete surgical resection if the mass is large or is causing symptoms. The most appropriate surgical approaches are posterior, anterior and lateral. Each has potential benefits and risks. Unfortunately, complete resection is not always possible as vertebral anomalies or extensive neural adhesion can make surgery difficult and hazardous. However, the cyst can be completely removed if it is situated in the extramedullary compartment with a clear plane of dissection between the lesion and neural elements [2–4].
Finally, thalamic infarction may be caused by arterial or venous infarcts. The thalamus plays an important role in awareness level and arousal regulation. Damage to the thalamus can cause memory loss, vertical gaze palsy, confusion and coma. The thalamus is supplied with blood by arteries including the tuberothalamic, paramedian, thalamogeniculate and posterior choroidal arteries. Vascular distribution varies by thalamic territory resulting in different symptoms depending on the territory infarcted [5].