EJCRIM 2023 CiteScore
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |
Last updated on 05 March, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 1213
HTML: 624
PDF: 524
|
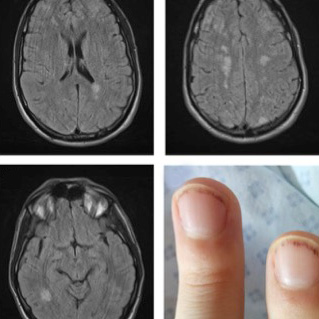
AFIP1L1-PDGFRA fusion can only be confirmed through molecular and cytogenetic investigations causing a delay in the diagnosis. However, patients with this mutation need urgent treatment because they present hypereosinophilia which may be associated with short-term tissue damage. Thromboembolism is a known cause of death in hypereosinophilic syndrome. A case of Loeffler endocarditis due to FIP1L1-PDGFRA-associated chronic eosinophilic leukemia presenting hemiparesis with fever, which also mislead the initial diagnosis, is reported.
|
Views: 1224
HTML: 173
PDF: 355
Figures 1-3: 0
Learning Points: 0
|
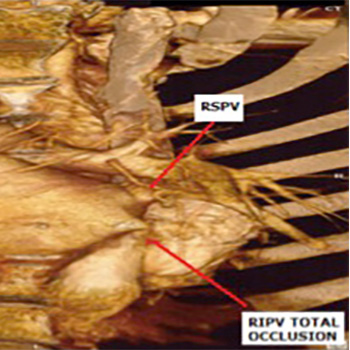
Introduction: A 47-year-old Caucasian woman with a past medical history of multiple ablative procedures for supraventricular arrhythmias and pacemaker implantation presented with increasing shortness of breath. The initial working diagnosis of the team treating her was ablation-induced pulmonary stenosis, especially after the recording of increased flow velocities through the right lower pulmonary vein.
Case presentation: The patient was alert and oriented, but obviously dyspnoeic. The vital signs were normal. The physical examination revealed a soft cardiac systolic murmur and the lungs were clear on auscultation. The electrocardiogram showed a pacemaker rhythm. The echocardiogram showed borderline normal global systolic function of the left ventricle and severe mitral regurgitation. The transoesophageal echocardiogram confirmed the above findings and revealed increased velocities through the right lower pulmonary vein. The working diagnosis of ablation-induced pulmonary stenosis was reinforced by the cardiac CT angiography. The patient was subsequently referred for surgical intervention. The intra-operative findings were both unexpected and impressive: congenital partial absence of the pericardium was responsible for herniation of the right chambers into the pleural space. Mitral regurgitation was attributed to failure of coaptation due to the very short surface of the leaflets. Extensive external fibrosis around the pulmonary veins caused the pulmonary vein stenosis.
Conclusion: The final diagnosis of a partial pericardial defect causing torsion and distortion of the heart chambers was made only at surgery. The consistent finding of pulmonary vein stenosis in the non-invasive modalities and the past medical history of ablations initially misleadingly led us to the assumption that they were related.

|
Views: 1794
HTML: 1203
PDF: 602
|
In 1934 Lemmel was the first to report the presence of juxtapapillary diverticula and hepatocholangiopancreatic disease, excluding cholelithiasis. Obstructive jaundice caused by periampullary duodenal diverticulum (PAD) in absence of choledocholithiasis or tumor is known as Lemmel syndrome. A patient with an extraluminal duodenal diverticulum presenting with obstructive jaundice and pancreatitis is presented in this case. Although initially managed conservatively, the patient had recurrence of symptoms after 2 months but then had successful surgical resection of the duodenal diverticulum.
|
Views: 1445
HTML: 615
PDF: 405
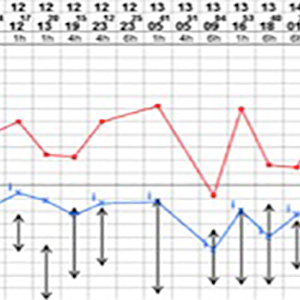
This figure shows the patient’s persistent pyrexia and other vital signs over the first five days of her admission.: 0
|
A 34 year-old Afro-Caribbean female presented with recurring episodes of fever and lower abdominal pain over a period of two months not improving despite courses of antibiotics for possible recurrent urinary tract infections. On admission to hospital, patient was treated for a possible pyelonephritis or pelvic inflammatory disease (PID). Extensive investigations into possible source of infection were carried out. However, all of the repeated microbiological cultures were normal. Patient was investigated further for other possible causes including connective tissue disease, haematological disorders, or neoplasm, all of which were normal. Diagnosis of adult onset Still’s disease (AOSD) was confirmed by a rheumatologist based on Yamaguchi’s diagnostic criteria for AOSD alongside significantly raised serum ferritin. Patient was treated with steroids to which she showed remarkable clinical improvement alongside marked reduction in her serum ferritin levels.
|
Views: 1132
HTML: 284
PDF: 530
PICTURES: 0
manuscript: 0
Untitled: 0
|
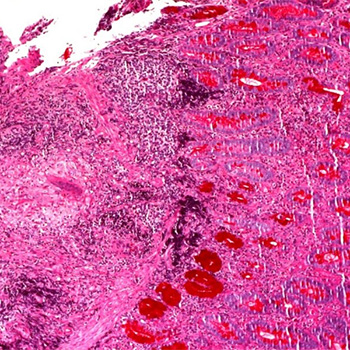
Aortitis results from aortic inflammation, frequent causes being infections and rheumatological disorders. The authors report the case of a 33-year-old black male with recent arterial hypertension, who presented with recurrent abdominal pain, jaundice, anorexia, weight loss and diarrhoea. Laboratory work-up was compatible with inflammatory anaemia and obstructive jaundice, while abdominal imaging revealed a dilated biliary tract, no visible gallstones, cephalic pancreatic globosity and aortic thickening. Pancreatic aspirate was negative for malignant cells, bacteria and Mycobacterium tuberculosis. The jaundice spontaneously subsided and the pancreatic globosity improved over time. Following positive PPD and IGRA, isoniazid was started. However, follow-up investigations revealed a severe bulbar stenosis with intense eosinophilic infiltrate, multiple non-necrotizing granulomas, and thoracic and abdominal aortitis not previously recognized. Immunological profile (ECA, ANCA and IgG4), eggs and parasites in stool samples were negative. The multisystemic disease, with an insidious and migrating behaviour, gastrointestinal and vascular involvement, granulomatous inflammatory response and tissue eosinophilia, raised the suspicion of a parasitic infestation (despite negative screening) or vasculitis. After 7 days of empirical treatment with albendazole and ivermectin, the patient passed a specimen of Ascaris lumbricoides in the stool and improved clinically.

|
Views: 2585
HTML: 2353
PDF: 766
Untitled: 0
Untitled: 0
Page 1: 0
Figure 1: 0
The learning points: 0
The learning points: 0
|
Background: Mercury is a highly toxic environmental metal that exists in three different forms: elemental, inorganic and organic. Intoxication occurs in either occupational or non-occupational settings, mainly after the inhalation of vapour and fumes in work places, laboratories or homes. Chronic mercury toxicity ranges from mild and insignificant to severe and life-threatening. We describe the case of a young male patient who presented with multiple organ dysfunction after chronic mercury exposure.
Case presentation: We report the case of 28-year-old male artisanal gold miner who was admitted to hospital for severe neurological impairment associated with inflammatory bowel disease-like symptoms and a skin rash after mercury exposure. Symptomatic treatment and corticosteroid administration assured rapid clinical improvement. Chronic mercury poisoning can masquerade as an autoimmune or systemic inflammatory disease.
Conclusion: Physicians should be aware that low exposure to mercury, even from artisanal gold mining, may be harmful to health. Management can be simple without the need for aggressive or invasive therapeutic measures. Larger case series are required in order to establish a clear management plan.
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2023, Published by SMC Media srl, Italy - Privacy policy