EJCRIM 2023 CiteScore
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |
Last updated on 05 April, 2024
Updated monthly
Updated monthly
Powered by




|
Views: 1035
HTML: 280
PDF: 390
Figure 1a: 0
Figure 1b: 0
Figure 1c: 0
|
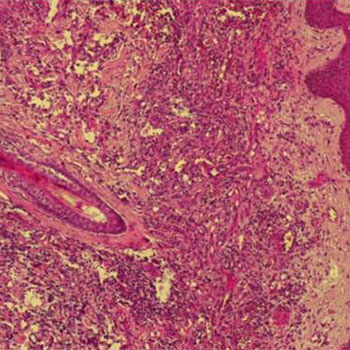
A patient presented with sudden, unexplained lower abdominal pain without peritonism or signs of infection or inflammatory reaction, but with recent bloody stools and a history of radiation therapy, diabetes and immunosuppression. Plain abdominal x-ray showed only air-fluid levels and air distention of the colon, but a later abdominal CT scan revealed extensive gas gangrene of the colon. The patient’s clinical status rapidly worsened. Elective surgical rectosigmoid debridement did not prevent the patient’s death. In conclusion, the diagnosis of ‘spontaneous’ life-threatening gas gangrene requires a high degree of clinical suspicion and allows life-saving surgical intervention.
|
Views: 1240
HTML: 758
PDF: 497
Photo 1: 0
Photo 2: 0
Photo 3: 0
Photo 4: 0
|
Introduction: Kaposi’s sarcoma (KS) is an angioproliferative disorder first described in 1872 by Moritz Kaposi. Four main clinical presentations of KS have been described: classic, endemic, iatrogenic and epidemic. KS involvement of the lymph nodes is extremely uncommon in the classical variant form, especially if it precedes the skin manifestations. We describe the case of an elderly HIV-negative patient presenting with lymphadenopathy who was found to have KS.
Case Report: A 67-year-old patient was admitted for exploration of polyadenopathies in the context of a general decline in health. Physical examination revealed an erythematosus left lower limb rash associated with angiomatous nodules and multiple lymphadenopathies. The diagnosis of erysipelas in the left leg was retained and the patient was treated with good evolution of the rash but persistence of the angiomatous nodules and the polyadenopathies. Skin and lymph node biopsies led to a diagnosis of KS. The patient is proposed for polychemotherapy.
Conclusion: KS must be suspected in lymphadenopathies despite the absence of typical cutaneous signs of the disease and in immunocompetent patients.
|
Views: 1033
HTML: 283
PDF: 455
Untitled: 0
Untitled: 0
Figure 2: 0
Figure 1: 0
|
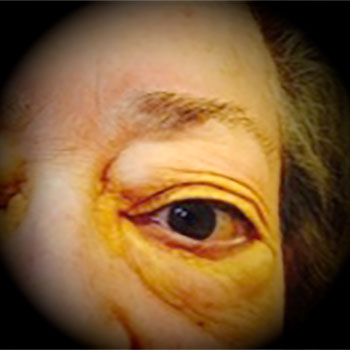
Erdheim-Chester disease (ECD) is a non-Langerhans’ histiocytosis and a very rare multisystemic disease of unknown aetiology, with skeletal involvement of the long bones and in more than 50% of cases with extraskeletal involvement. The disease was described in 1930 by the anatomopathologist Jakob Erdheim and his student William Chester. More than 500 cases have since been reported. We report the case of a 77-year-old Italian woman with ECD who was admitted to hospital for acute cardiac tamponade. The patient presented with simultaneous cutaneous, retro-orbital, skeletal, cerebral and cardiovascular manifestations and was successfully treated with corticosteroids followed by interferon.

|
Views: 1128
HTML: 369
PDF: 459
Figure 3: 0
Figure 1: 0
figure 2: 0
|
Introduction: Thrombosis has been widely reported in coeliac disease (CD) but central retinal vein occlusion (CRVO) is rarely described.
Case presentation: A 27-year-old woman presented with acute visual loss and was diagnosed with CRVO. Her protein S and protein C levels were low and CD was diagnosed on the basis of endoscopic, immunological and histological results. A gluten-free diet resulted in favourable evolution.
Conclusion: CD should be considered in young patients with thrombosis, especially if in an unusual location. Treatment is based on a gluten-free diet.
|
Views: 976
HTML: 239
PDF: 364
Untitled: 0
Untitled: 0
|
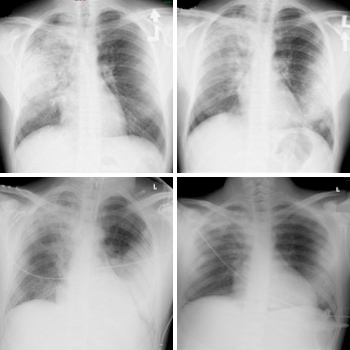
A 21-year-old male patient with a history of occupational exposure to open fire smoke was initially treated with empiric antibiotics for simple community-acquired pneumonia. However, he continued to deteriorate rapidly, developed respiratory failure and needed mechanical ventilation. After possible aetiologies were considered, acute eosinophilic pneumonia was suspected and confirmed by broncho-alveolar lavage. His condition improved dramatically soon after glucocorticoid administration and he was discharged without sequelae. Acute eosinophilic pneumonia should be considered in a patient with a history of exposure to smoke presenting with pneumonia that deteriorates rapidly despite broad antibiotics. An important clue for the diagnosis is eosinophilia in peripheral blood.

|
Views: 1144
HTML: 807
PDF: 411
Figure 2: 0
Figure 1: 0
|
We present a case of an elderly woman with long-term indwelling urinary catheter use whose urine turned purple due to a urinary tract infection.

|
Views: 1125
HTML: 321
PDF: 394
Figure 1: 0
Figure 2: 0
Figure 5: 0
Figure 4: 0
Figure 3: 0
Pictures Captions: 0
Pictures Captions: 0
|
A 63-year-old male patient suffered from myalgia, arthralgia cough and erythematous macules, with confluence to the thorax, limbs, thighs and the scrotum. The erythematous macules evolved to blisters with a positive Nikolsky’s sign. A cutaneous biopsy revealed satellite cell necrosis. Administration of immunoglobulins resulted in a favourable evolution of the cutaneous lesions. Toxic epidermal necrolysis (TEN) is a rare and potentially fatal mucocutaneous disease. Early recognition, diagnosis and therapy are of the utmost importance.

|
Views: 1226
HTML: 1290
PDF: 402
|
Porphyrias are a group of disorders caused by enzymatic defects in the biosynthesis of haem. Congenital erythropoietic porphyria (CEP) or Günther's disease is an extremely rare autosomal recessive disorder. Clinical manifestations include onset in infancy of blistering of sun-exposed areas, atrophic scars, mutilated fingers, and bright red fluorescence of the urine and teeth without neurological involvement. The only available prophylactic treatment for CEP is total avoidance of sunlight. A high degree of suspicion is required for the diagnosis. Early diagnosis is very important to prevent subsequent damage.
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2023, Published by SMC Media srl, Italy - Privacy policy