EJCRIM 2023 CiteScore
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |
Last updated on 05 March, 2024
Updated monthly
Updated monthly
Powered by



|
Views: 1103
HTML: 248
PDF: 465
Figure 2: Clinical autopsy: 0
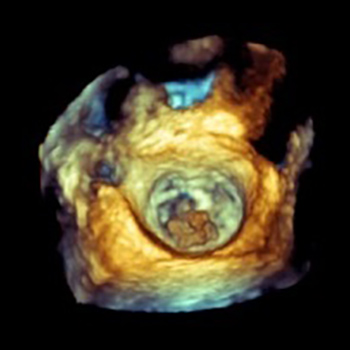
Figure 1. Transesophageal echocardiography showing vegetation on the mitral valve: 0
|
We describe the case of a 68-year-old man, who presented with an ischemic stroke due to cardiac embolization related to mitral valve endocarditis. Blood cultures were always negative and post-operative valve histology did not show microorganisms. The patient also presented further recurrent peripheral embolic events. These clinical aspects were the first sign of a pancreas adenocarcinoma, which was only diagnosed in the clinical autopsy. In conclusion, these clinical findings of recurrent thromboembolic events with no microorganisms isolated suggests the diagnostic of a marantic endocarditis.
|
Views: 1104
HTML: 216
PDF: 365
Figure 1: 0
Figure 2: 0
Figure 3: 0
|
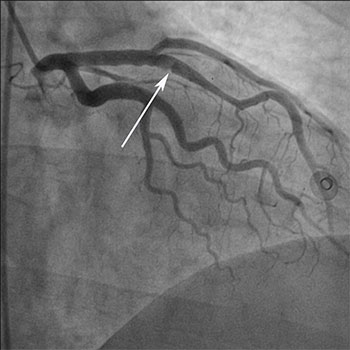
We report here the case of a young patient with a simultaneous isolated septal myocardial infarction (MI) and pulmonary embolism (PE).
The aim was to describe a rare clinical entity and to explain why these two pathologies were present at the same time in a young patient.?
A review of literature was established. An interventional cardiologist, an interventional radiologist and a lung specialist were consulted.
The diagnostic workup revealed only heterozygous Factor Leiden V mutation. This presentation was probably fortuitous, but worth reporting to our opinion.
|
Views: 1412
HTML: 512
PDF: 434
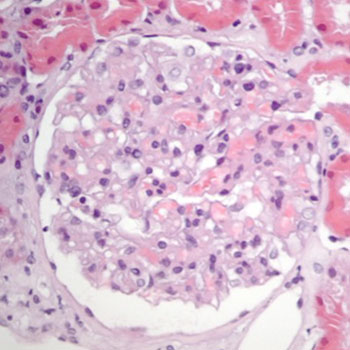
A rare presentation of leptospirosis: 0
|
Leptospirosis has a wide spectrum of clinical manifestations. Acute renal failure, an important complication, generally involves interstitial and tubular damage. We describe the case of a 42-year-old man who was admitted with fever, back pain and periorbital oedema. He had hypertension, thrombocytopenia, acute renal failure, hypoalbuminaemia, hypertriglyceridaemia and proteinuria >4.00 g/l. The renal biopsy showed mesangioproliferative glomerulonephritis. Due to the epidemiological context and clinical picture, ceftriaxone was started with rapid clinical improvement. Blood PCR for leptospira came back positive. The presentation of leptospirosis as nephrotic syndrome is rare and this diagnosis should be considered before performing a renal biopsy.

|
Views: 1196
HTML: 610
PDF: 420
|
We report a case of paradoxical deterioration. A male patient diagnosed with pleural tuberculosis, but who was not infected with human immunodeficiency virus (HIV), experienced clinical deterioration 3 weeks after the initiation of anti-tuberculous treatment. After other diagnoses were ruled out, a paradoxical response to treatment was established and the patient was started on systemic corticosteroids. Paradoxical response to treatment should be considered in patients with clinical deterioration after they start on anti-tuberculous treatment.

|
Views: 1233
HTML: 276
PDF: 362
Authors' disclosure and copyright authorization form: 0
Figure 1: 0
|
We present the first case of gastro-intestinal perforation caused by a mint twig decorating a cocktail drink. A 76-year-old man was enjoying his Mojito cocktail on a cruise ship near Mexico when he accidently swallowed a mint twig, resulting in ileum perforation. This led to a cascade of events, eventually resulting in life-threatening multi-organ failure. Given this rare but potentially severe complication and the increasing popularity of decorated drinks, a less ‘fancy’ presentation for cocktails and similar drinks may be warranted.
|
Views: 907
HTML: 181
PDF: 332
|
We report the case of a 67-year-old man who was admitted to our Intensive Care Unit because of traumatic brain injury. During his prolonged hospitalization, gradual darkening of the skin all over his body was observed. An excess corticotropin (ACTH) production syndrome was considered. The patient’s hormone study showed high levels of ACTH (978 pg/ml) with normal cortisol levels. Extensive clinical and laboratory investigations revealed adenocarcinoma of the colon, which was likely the site of the ectopic ACTH production. This is a very rare manifestation of paraneoplastic syndrome during the course of colon adenocarcinoma. The most important feature of this case report is that this rare syndrome was accidentally discovered, in a patient hospitalized for unrelated reasons, by simple clinical investigation.

|
Views: 2091
HTML: 529
PDF: 603
Figure 1 (CTPA): 0
Figure 2 (CT Aortogram): 0
Figure 3 (CT Aortogram): 0
TABLE 1. Risk Conditions for Aortic Dissection: 0
|
Thoracic aortic dissection (TAD) has a very high mortality rate and is often missed due to the atypical presentation of patients. We present a case of a man with chronic hypertension, atrial fibrillation (AF) (on regular warfarin) and a previous endovascular aneurysm repair (EVAR), who presented with dyspepsia and was incidentally found to have a ruptured distal thoracic aneurysm on imaging with no obvious clinical signs on examination, nor abnormalities on admission chest x-ray (CXR).
|
Views: 2050
HTML: 1966
PDF: 603
Figure 1: 0
Figure 2: 0
Figure 2: 0
Figure 3: 0
Table 1: 0
Learning Points: 0
|
Acute cholecystitis after colonoscopy is a rare event, with less than 10 cases described in the literature. We report the case of a male patient with silent gallstones who underwent colonoscopy for follow-up of his Crohn’s disease. The colonoscopy revealed erosions in the terminal ileum, from which biopsies were taken. A sessile polyp 4 mm in diameter at the recto-sigmoid junction was also removed. Less than 24 h after the colonoscopy, the patient complained of upper right quadrant pain, nausea and vomiting. Based on the clinical findings, laboratory data and ultrasonography, we diagnosed acute cholecystitis and excluded any complication after the colonoscopy. Laparoscopic cholecystectomy was performed and the patient was discharged.
| 2.1 = | 1.730 Cit. to date |
| 842 Docs. to date |




Publisher
Official Journal of the
European Federation of Internal Medicine
www.efim.org
Publisher: SMC media Srl
Via Giovenale, 7 - 20136 Milan - Italy
P.IVA 07626490960
info@ejcrim.com
www.ejcrim.com - ISSN: 2284-2594 - © EFIM 2014-2023, Published by SMC Media srl, Italy - Privacy policy