Keywords
coronary artery fistula, abberant coronary artery, cardiac CT, cardiac catheterization
Abstract
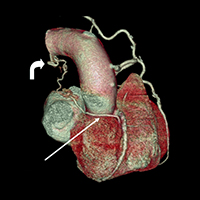
Coronary artery fistulae (CAF) are a rare entity describing abnormal communication between a coronary artery and cardiac chamber or a large intrathoracic vessel and are seldom described in the literature[1]. These fistulae can be either congenital or acquired. Often incidental in finding, CAFs can have serious clinical sequelae, and should be duly reported and discussed with the cardiac team. More than 50% of patients with CAFs may be asymptomatic; 34% may report chest pain; 13% may have symptoms of heart failure, and a minority of 2% may suffer from endocarditis and arrhythmias[2]. The largest series to our knowledge was reported by the Cleveland Clinic, which found 225 patients with incidental CAF out of 126,595 coronary catheterizations (incidence of 0.18%), performed during a span of 28 years [3].
Multiple CAFs are an even rarer entity and only a handful of cases have been reported in the literature to date. Few cases of double CAFs have been reported that describe two different feeder coronary arteries giving rise to separate drainage sites[3]. In our report, however, we describe a new entity: a single-feeder coronary vessel communicated with two drainage sites. Our case is curiously unique, in which we report a single artery, originating from the right coronary artery (RCA) with double drainage sites – one to the left pulmonary artery and the second to the left bronchial artery.
References
Views: 754
HTML downloads: 231
PDF downloads: 359
Published:
2015-04-13
Issue:
Vol. 2 No. 2 (2015)
(view)