ABSTRACT
Objectives: To describe brucellosis and its possible complications according to clinical, laboratory and radiological findings.
Methods: We describe a case of
Results: Clinical manifestations, imaging and laboratory findings provided the correct diagnosis of Brucella pericarditis. The patient recovered fully following doxycycline and rifampin therapy.
Conclusion: Brucellosis should be considered in the differential diagnosis of disorders that affect the pericardium in endemic areas.
LEARNING POINTS
- Brucella pericarditis should be considered in case of disorders that affect the pericardium in endemic areas such as the Mediterranean region.
- When a patient has been diagnosed with brucellosis, oral doxycycline 100 mg twice daily plus oral rifampin 600 mg once daily must be given immediately.
KEYWORDS
Brucellosis, pericarditis; infectious disease.
INTRODUCTION
Brucellosis is a zoonotic disease which is a systemic infection with a broad clinical presentation ranging from asymptomatic to severe disease. Brucella infection can affect any organ and system in the human body. The spleen, liver, bone marrow and reticuloendothelial cells are the most frequently affected, with cardiovascular involvement, such as endocarditis, pericarditis and myocarditis, being extremely rare. Here we describe a patient with Brucella infection complicated with Brucella pericarditis in the absence of concomitant endocarditis, diagnosed as a result of clinical manifestations, imaging, laboratory findings including culture and serology, and the patient's occupation.
CASE DESCRIPTION
A 50-year-old man was admitted our hospital with fever, malaise, night sweats and chest pain. He had no medical history and lives in Turkey's Mediterranean region. He works on a farm and consumes his own milk, cheese and yogurt. Physical examination revealed a temperature of 38.7ºC, a cardiac murmur and tachypnoea. Laboratory investigations showed a normal complete blood count, high levels of C-reactive protein (40 mg/l) and an erythrocyte sedimentation rate of 57. Electrocardiography was normal, while transthoracic echocardiography showed pericardial effusion (pericardial thickness of 2.3 cm) without cardiac tamponade, normal valves and no signs of endocarditis (Fig. 1). Computed tomography of the thorax also showed pericardial effusion (Fig. 2). Tests for anti-
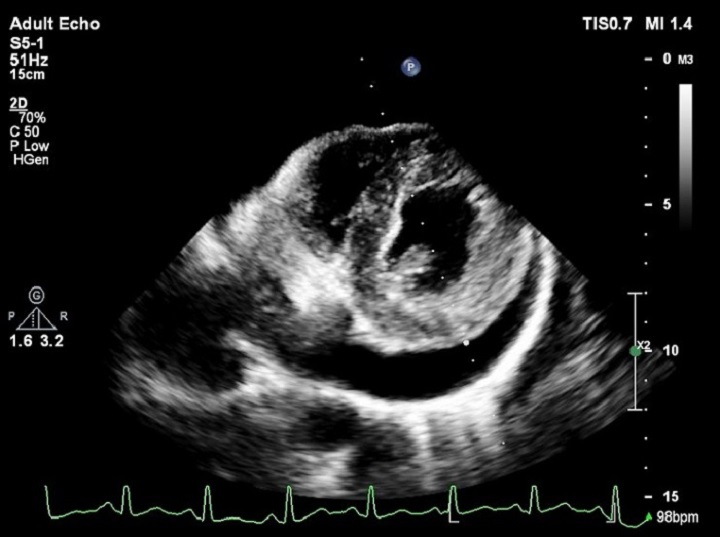
Figure 1 (click to enlarge)

Figure 2 (click to enlarge)
Figure 1. Transthoracic echocardiography image of pericardial effusion
Figure 2. Thoracic computed tomography image of pericardial effusion
DISCUSSION
Brucellosis is zoonotic infection with a high prevalence in the Mediterranean region. Brucella spp. can be transmitted to humans from infectious animals and cause disease in humans[1]. The clinical presentation of brucellosis ranges from asymtomatic to severe disease and includes haematological, gastrointestinal, osteoarticular, neurological and cardiovascular complications[2]. Cardiovascular problems such as myocarditis, endocarditits and pericarditis are rarely seen. Myocarditis is the most common cardiac complication of brucellosis[3]. Gür et al. found endocarditis, with concomitant myocarditis and pericarditis, in only two of 283 cases[4]. In another study from Spain, isolated Brucella pericarditis was detected in only one patient out of 530 cases[5]. This patient worked as a farmer and had a history of fever, night sweats, malaise and chest pain. Transthoracic echocardiogarphy showed pericardial effusion (2.3 cm thickness) without cardiac tamponade. A report by Gatselis et al. described two cases of Brucella pericarditis identified by blood culture[6]. In our case, Brucella spp. were isolated from blood cultures and tests for anti-Brucella IgG and IgM were strongly positive, as was a standard tube Rose Bengal agglutination test specific for brucellosis (titre >1/640). We conducted additional tests which ruled out other causes of pericardial effusion.
Consequently, a diagnosis of Brucella pericariditis was made. We did not perform pericardiocentesis, because in the absence of cardiac tamponade, this procedure is not essential in cases of Brucella pericarditis[2]. In the absence of heart failure or valvular destruction, some cases have been treated with only antibiotic combinations[7]. Our patient was put on combined antibiotic therapy (doxycycline and rifampin), his signs and symptoms regressed and regular follow-up was conducted.
CONCLUSION
Brucellosis is highly prevalent in the Mediterranean region. This patient's history of exposure and clinical manifestations suggested Brucella infection. Brucellosis should be considered in the differential diagnosis of disorders that affect the pericardium in endemic areas. Clinical suspicion, adequate antibiotic treatment and a multidisciplinary approach result in complete cure in brucellosis where the main cause of death is heart disease.