ABSTRACT
Objectives: Breast carcinoma with choriocarcinomatous differentiation is a rare entity, generally presenting with high-grade disease and an aggressive clinicalcourse with overall survival of less than a year
Case: A 69-year-old woman with a diagnosis of pT1N0M0 invasive ductal carcinoma with choriocarcinomatous differentiation received six cycles ofadjuvant chemotherapy and is still disease free on the 23rd month after diagnosis, showing a better prognosis than most other cases reported in theliterature.
Conclusion: The reason for the poor prognosis for this type of breast carcinoma remains unclear. Standard chemotherapeutic agents administered for breastcarcinoma may be used for choriocarcinomatous differentiation.
LEARNING POINTS
- Breast carcinoma with choriocarcinomatous differentiation is a rare entity.
- An uncommonly long disease-free survival has been observed in this case.
- To our knowledge, this is the first report of a specific chemotherapy regimen for this rare subtype.
KEYWORDS
Breast carcinoma, choriocarcinomatous differentiation, chemiotherapy
BACKGROUND
Choriocarcinomatous differentiation has been described previously in tumours of the bladder, oesophagus and colon[1,3], but it is quite rare in breast carcinomas. Breast carcinoma with choriocarcinomatous features was first described by Saigo and Rosen in 1981[4]. They described a 55-year-old patient with a breast tumour that contained mono- and multinucleated giant cells strongly resembling a choriocarcinoma ofgestational trophoblastic origin. A limited number of such cases have been reported. Most of them presented with high-grade disease, exhibiting anaggressive clinical course with an overall survival of less than a year[5,6]. However, in two cases, 2 and 4 years of disease-free survival were reported[7]. We report an additional case of breast carcinoma with choriocarcinomatous features and a brief review of the literature.
CASE
A 69-year-old woman presented with a left breast mass. The initial mammogram showed a left breast lesion of 21×17 mm with irregular borders. The patient underwent a modified left radical mastectomy with axillary dissection. Microscopically, the 2×1.5 cm tumour mass consisted of solid nests and anastomosing cords of tumour cells separated by sparse cellular desmoplastic stroma, suggestive ofinvasive ductal carcinoma. Most, if not all, of the tumour consisted of choriocarcinomatous differentiation areas composed of groups of a few mono- andmultinucleated syncytiotrophoblast-like giant cells, which looked like choriocarcinoma cells.
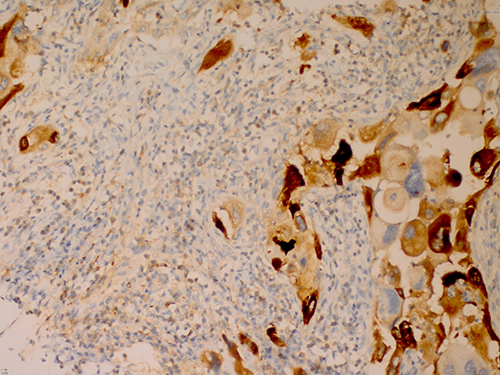
Figure 1 (click to enlarge)
Fig. 1 - Immunohistochemical staining with hCG in the cells
No intraductal carcinoma and no lymphovascular invasion were detected,whereas perineural invasion was present.Immunohistochemically, thechoriocarcinomatous differentiation areas stained positively for humanchorionic gonadotropin (hCG) (Fig. 1) and placental alkalinephosphatase (PLAP), while the tumour stained negative for ER, PR andcerbB2. The 14 lymph nodes extracted from thespecimen were negative forcarcinoma infiltration.
Imaging results were negative for systemic metastases. The diagnosis was pT1N0M0 invasive ductal carcinoma withchoriocarcinomatous differentiation.
Adjuvant chemotherapy, the same as that used for the equivalent stage of breast carcinoma, consisting of 6 cycles ofCAF (cyclophosphamide 500 mg, doxorubicin 50 mg, 5-FU 500 mg per square metre of body surface area) was administered.
Twenty-three months after diagnosis, the patient is still disease free.
CONCLUSION
Breast carcinoma with choriocarcinomatous features is a rare variant of breast malignancy, usuallyassumed to have a poor prognosis and poor response to treatment. However, it is difficult to assess the efficacy of treatment for this condition because of itsrarity and occasional reports of good outcomes.
These tumours are composed of atypical malignant cells, similar to choriocarcinoma cells, that can express hCG and humanplacental lactogen markers[8]. In some cases, isolated carcinoma cells that are reactive immunohistochemically for hCG can be found in 5–21% of common invasiveductal carcinoma of the breast without choriocarcinomatous features. It has been shown that the presence of such non-choriocarcinomatous cells reactive forhCG does not carry any prognostic significance and clinical importance[9].
Another differential diagnosis is with carcinoma metastatic to the breast. This is also a rare event and most caseshave a history of hydatiform mole or choriocarcinoma[10,11]. In breast carcinoma with choriocarcinomatous differentiation, there is usually a negativehistory for gynaecologic malignancies, and invasive or in situ ductal areas are important markers for diagnosis. In this case, there were areas of choriocarcinomatous differentiation intermingled withinvasive ductal carcinoma.
There are limited numbers of these cases in the literature and most patients were reported to be peri- or postmenopausal,as was our patient[6,7]. However, three cases in their 30s and one in the fifth week of pregnancy have also been reported[5,12,13]. In the literature, a rightbreast predilection was reported. However, in our case the tumour was located in the left breast[12,14]. In two cases, only positivity for ER and/or PRstaining were reported, although these were negative in our case[7,15]. All but one case was shown to have invasive ductal carcinoma accompanying achoriocarcinomatous pattern, as in our patient. Green reported a case with primary colloid carcinoma showing focal choriocarcinomatous features[16].
This case was diagnosed at an earlier stage and has had a longer disease-free survival than most cases reported inthe literature. The recommended treatment for this type of breast carcinoma is surgical resection, the same as in conventional breast carcinoma with the samestage at diagnosis. There is no established chemotherapy regimen. We chose a chemotherapy regimen commonly used in the same stage of breast carcinoma.Generally, patients have been reported to present with locally advanced stage and lymph node and distant metastases. Most died within 1 year of diagnosis[4,5,12]. However, Erhan et al. reported two of four cases of breast carcinoma with choriocarcinomatous features had a disease-free survival of 2 and 4 years[7]. Resetkova et al. reported two cases; one of them (a 38-year-old woman in her fifth week of pregnancy) was disease free after one year[12]. Clearly, morereports from other clinicians who have managed this rare tumour subtype are needed in order to establish its optimal treatment.